Das könnte Ihnen auch gefallen
- Case Study On NSVDDokument50 SeitenCase Study On NSVDNyj Quiño100% (2)
- Case Study Cesarean-SectionDokument13 SeitenCase Study Cesarean-SectionRenelli Anne Gonzaga100% (2)
- Case Study of Cesarean SectionDokument9 SeitenCase Study of Cesarean Sectionzarian wu72% (18)
- Cesarean Section CaseStudyDokument23 SeitenCesarean Section CaseStudyDada Malicsi LandichoNoch keine Bewertungen
- Cesarean Delivery Case Presentation ConceptualDokument57 SeitenCesarean Delivery Case Presentation ConceptualHope Serquiña67% (3)
- Cesarean Section Case StudyDokument3 SeitenCesarean Section Case StudyMitch RendonNoch keine Bewertungen
- Cesarean SectionDokument22 SeitenCesarean SectionKarlo Bartolome100% (2)
- Case StudyDokument45 SeitenCase StudykimJCANoch keine Bewertungen
- Case Study CS 3Dokument38 SeitenCase Study CS 3tristanpaulNoch keine Bewertungen
- Cs - Cesarean SectionDokument19 SeitenCs - Cesarean Sectiondaph-me75% (16)
- Nursing Case Study C SectionDokument12 SeitenNursing Case Study C SectionRiojane75% (8)
- Cesarian Section Case PresentationDokument26 SeitenCesarian Section Case PresentationMae Azores86% (51)
- Case StudyDokument17 SeitenCase StudyLourd Andrew VillegasNoch keine Bewertungen
- C-Section Case StudyDokument4 SeitenC-Section Case StudyChin Villanueva Ulam0% (1)
- Care Study CAESARIAN SECTIONDokument29 SeitenCare Study CAESARIAN SECTIONNoreen EndinoNoch keine Bewertungen
- CASE STUDY Cesarean DeliveryDokument15 SeitenCASE STUDY Cesarean Deliverydirkdarren100% (3)
- CS Case StudyDokument31 SeitenCS Case StudyAira MiyaNoch keine Bewertungen
- Surgical Cs Case Study - BangDokument25 SeitenSurgical Cs Case Study - BangClyde R.OrtegaNoch keine Bewertungen
- Case Study - NSVD ScribdDokument20 SeitenCase Study - NSVD ScribdShar EnriquezNoch keine Bewertungen
- Case Study: Lower Segment Caesarean SectionDokument9 SeitenCase Study: Lower Segment Caesarean SectionaliasLiew100% (3)
- A Case Study of Cesarean Delivery (Breech Presentation) : Submitted By: Corpus. NichelleDokument25 SeitenA Case Study of Cesarean Delivery (Breech Presentation) : Submitted By: Corpus. NichelleAnne MauNoch keine Bewertungen
- Placenta Previa Case StudyDokument59 SeitenPlacenta Previa Case StudySiergs Smith GervacioNoch keine Bewertungen
- Uterine RuptureDokument19 SeitenUterine RuptureAna Denise Quinajon0% (1)
- Group 2. Ectopic PregnancyDokument61 SeitenGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
- Uterine ProlapseDokument44 SeitenUterine ProlapseMoi Mendoza83% (6)
- Cesarean SectionDokument16 SeitenCesarean Sectionjannnjennn67% (3)
- Case Study-Cesarean BirthDokument5 SeitenCase Study-Cesarean BirthDada Malicsi Landicho100% (2)
- Multifetal Gestation Case StudyDokument67 SeitenMultifetal Gestation Case StudyNikki Joy NavarroNoch keine Bewertungen
- CASE ANALYSIS Ectopic Pregnancy Part 1Dokument10 SeitenCASE ANALYSIS Ectopic Pregnancy Part 1Diane Celine SantianoNoch keine Bewertungen
- Case Study MiscariageDokument14 SeitenCase Study MiscariagesexiiimammaNoch keine Bewertungen
- Case Study Placenta PreviaDokument19 SeitenCase Study Placenta Previajeanette_03100% (1)
- Case Study - Ectopic PregnancyDokument10 SeitenCase Study - Ectopic Pregnancykristine keen buanNoch keine Bewertungen
- NSVDDokument48 SeitenNSVDchiqui14100% (2)
- Case Study Placenta Previa This Is It 1Dokument71 SeitenCase Study Placenta Previa This Is It 1Homework Ping100% (1)
- Hospital Case Study 2nd Sem.Dokument22 SeitenHospital Case Study 2nd Sem.Salvador V Quindipan JrNoch keine Bewertungen
- Placenta Previa Case StudyDokument59 SeitenPlacenta Previa Case Studyjuel_navarro88% (33)
- EctopicDokument41 SeitenEctopicVillanueva Ameera MaeNoch keine Bewertungen
- Placenta Previa Case StudyDokument59 SeitenPlacenta Previa Case StudyKen KenNoch keine Bewertungen
- Normal Spontaneous Vaginal DeliveryDokument41 SeitenNormal Spontaneous Vaginal DeliveryTina Talmadge100% (1)
- Uterine MyomaDokument43 SeitenUterine MyomaJeselo Ouano Gorme100% (1)
- Case Study of Cesarean SectionDokument9 SeitenCase Study of Cesarean SectionErika Joy Imperio0% (1)
- Normal Spontaneous DeliveryDokument21 SeitenNormal Spontaneous Deliverygeelawliet100% (4)
- Case Study (Placenta Previa) This Is It!!!Dokument68 SeitenCase Study (Placenta Previa) This Is It!!!Joeren Gonzales86% (14)
- Case Study (NSD - Primi)Dokument29 SeitenCase Study (NSD - Primi)Kimberly Anne SP Padilla82% (11)
- Placenta Previa Case StudyDokument7 SeitenPlacenta Previa Case StudyphearlieNoch keine Bewertungen
- MS CaseDokument28 SeitenMS CaseJuwaka OsakaNoch keine Bewertungen
- Patient Profile: AST Edical IstoryDokument9 SeitenPatient Profile: AST Edical IstoryAkocmeme SanchezNoch keine Bewertungen
- NCMH Case Study 2Dokument22 SeitenNCMH Case Study 2Kristoff StJohn Gamilla CuasayNoch keine Bewertungen
- Aacase 2Dokument13 SeitenAacase 2Michele RogersNoch keine Bewertungen
- Vehicular AccidentDokument9 SeitenVehicular AccidentCharm TanyaNoch keine Bewertungen
- Case Pres )Dokument18 SeitenCase Pres )Justin Faye VibarNoch keine Bewertungen
- Final SDL 1Dokument21 SeitenFinal SDL 1Cy PilapilNoch keine Bewertungen
- Case Study On FCBDDokument38 SeitenCase Study On FCBDKwinutskie LiteratoNoch keine Bewertungen
- Thirteen Areas of Assessment I. PsychologicalDokument2 SeitenThirteen Areas of Assessment I. PsychologicalShehada Marcos BondadNoch keine Bewertungen
- CP AdriaticoDokument39 SeitenCP AdriaticoADRIATICO JAROSLUVNoch keine Bewertungen
- Nursing Process FormatDokument7 SeitenNursing Process FormatIssa FarneNoch keine Bewertungen
- Age - For SubmissionDokument27 SeitenAge - For SubmissionAdrian MallarNoch keine Bewertungen
- Incomplete AbortionDokument22 SeitenIncomplete AbortionAJ Dalawampu100% (2)
- Patient J.M.R Felt Numbness On His Left Lower ExtremityDokument6 SeitenPatient J.M.R Felt Numbness On His Left Lower ExtremityRaidis PangilinanNoch keine Bewertungen
- BPPV CaseDokument24 SeitenBPPV CaseAnonymous ZbVovJEFuNoch keine Bewertungen
- The Public Health System and The 10 Essential Public Health ServicesDokument2 SeitenThe Public Health System and The 10 Essential Public Health ServicesWeng Maesa MontemayorNoch keine Bewertungen
- About AppendicitisDokument3 SeitenAbout AppendicitisWeng Maesa MontemayorNoch keine Bewertungen
- Mannitol Drug StudyDokument2 SeitenMannitol Drug StudyKelly Riedinger100% (1)
- Impartial of Fulfillment in Cultural Anthropology: Arellano University 2600 Legarda St. MlaDokument2 SeitenImpartial of Fulfillment in Cultural Anthropology: Arellano University 2600 Legarda St. MlaWeng Maesa MontemayorNoch keine Bewertungen
- Unang YakapDokument9 SeitenUnang YakapWeng Maesa MontemayorNoch keine Bewertungen
- Pleural EffusionDokument3 SeitenPleural EffusionWeng Maesa MontemayorNoch keine Bewertungen
- 4m.case Study 2013Dokument4 Seiten4m.case Study 2013Weng Maesa MontemayorNoch keine Bewertungen
- TraumaDokument5 SeitenTraumaWeng Maesa MontemayorNoch keine Bewertungen
- Wilms TumorDokument2 SeitenWilms TumorWeng Maesa MontemayorNoch keine Bewertungen
- Emergency Drug KitDokument2 SeitenEmergency Drug KitWeng Maesa MontemayorNoch keine Bewertungen
- Anatomy and PhysiologyDokument4 SeitenAnatomy and PhysiologyWeng Maesa MontemayorNoch keine Bewertungen
- Theories of Labor OnsetDokument1 SeiteTheories of Labor OnsetWeng Maesa MontemayorNoch keine Bewertungen
- Arf 1Dokument28 SeitenArf 1Weng Maesa MontemayorNoch keine Bewertungen
- Git NursingDokument245 SeitenGit NursingWeng Maesa MontemayorNoch keine Bewertungen
- Principal Geriatric SyndromesDokument2 SeitenPrincipal Geriatric SyndromesWeng Maesa MontemayorNoch keine Bewertungen
- Commonly Asked Emergency DrugsDokument17 SeitenCommonly Asked Emergency DrugsrianneNoch keine Bewertungen
- Ectrin. Drug StudyDokument1 SeiteEctrin. Drug StudyWeng Maesa Montemayor100% (1)
- Arf 1Dokument28 SeitenArf 1Weng Maesa MontemayorNoch keine Bewertungen
- Generic NameDokument3 SeitenGeneric NameWeng Maesa MontemayorNoch keine Bewertungen
- Unang YakapDokument9 SeitenUnang YakapWeng Maesa MontemayorNoch keine Bewertungen
- Oxygen Therapy Is The Administration of Oxygen As A Medical Intervention, Which Can BeDokument3 SeitenOxygen Therapy Is The Administration of Oxygen As A Medical Intervention, Which Can BeWeng Maesa MontemayorNoch keine Bewertungen
- The Field Health Service Information System (FHSIS)Dokument22 SeitenThe Field Health Service Information System (FHSIS)i_love_quinn86% (56)
- ABC MsDokument62 SeitenABC MsWeng Maesa MontemayorNoch keine Bewertungen
- Acute Respiratory FailureDokument8 SeitenAcute Respiratory FailureCayunk NorlianaNoch keine Bewertungen
- Pharma 1Dokument11 SeitenPharma 1Weng Maesa MontemayorNoch keine Bewertungen
- Wilms TumorDokument2 SeitenWilms TumorWeng Maesa MontemayorNoch keine Bewertungen
- Principles of SterilityDokument4 SeitenPrinciples of SterilityCris SolandNoch keine Bewertungen
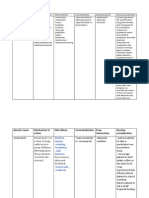
- Drug Name Drug Action Indication/ Dosage Contraindications Adverse Effects Drug Interactions Nursing ConsiderationsDokument1 SeiteDrug Name Drug Action Indication/ Dosage Contraindications Adverse Effects Drug Interactions Nursing ConsiderationsWeng Maesa MontemayorNoch keine Bewertungen
- Pathogenesis of Infectious DiseaseDokument2 SeitenPathogenesis of Infectious DiseaseWeng Maesa MontemayorNoch keine Bewertungen
- 0310 젠바디 COVID-19 리플렛Dokument2 Seiten0310 젠바디 COVID-19 리플렛Fara EsterNoch keine Bewertungen
- Illustrated Manual of Infectious Diseases of Livestock in AfghanistanDokument245 SeitenIllustrated Manual of Infectious Diseases of Livestock in Afghanistanqadir-qadis100% (2)
- 2000 - Solano-Gallego Et Al. - The Ibizian Hound Presents A Predominantly Cellular Immune Response Against Natural Leishmania InfectionDokument9 Seiten2000 - Solano-Gallego Et Al. - The Ibizian Hound Presents A Predominantly Cellular Immune Response Against Natural Leishmania Infectionvltg_35643Noch keine Bewertungen
- (Pediaii) - 021 - Disorders of The Respiratory TractDokument17 Seiten(Pediaii) - 021 - Disorders of The Respiratory TractdoktoraronaNoch keine Bewertungen
- 10995752Dokument14 Seiten10995752felipe_fismed4429Noch keine Bewertungen
- Hepatitis B & C & D VirusDokument14 SeitenHepatitis B & C & D VirusAtheer AlabdyNoch keine Bewertungen
- Covid-19 AddendumDokument10 SeitenCovid-19 AddendumPrecious Bardon-MempinNoch keine Bewertungen
- Basics of Stem Cell TransplantDokument46 SeitenBasics of Stem Cell TransplantNarendra Bhattarai100% (5)
- The Beck ProtocolDokument81 SeitenThe Beck ProtocolwxcvbnnbvcxwNoch keine Bewertungen
- Copyright © The McGraw-Hill Companies, Inc. Permission Required For ReproductionDokument33 SeitenCopyright © The McGraw-Hill Companies, Inc. Permission Required For ReproductionKvaleramNoch keine Bewertungen
- Bird Flu: "Av Ian I NF Luenz A"Dokument8 SeitenBird Flu: "Av Ian I NF Luenz A"Rayza MaglaqueNoch keine Bewertungen
- National Tuberculosis Control ProgramDokument3 SeitenNational Tuberculosis Control ProgrampeterjongNoch keine Bewertungen
- Ultima Forsan - A Taste of Macabre SWDokument31 SeitenUltima Forsan - A Taste of Macabre SWMaya Karasova100% (1)
- Acute Viral Gastroenteritis in Children in Resource-Abundant Countries - Clinical Features and Diagnosis - UpToDateDokument39 SeitenAcute Viral Gastroenteritis in Children in Resource-Abundant Countries - Clinical Features and Diagnosis - UpToDateDING TIAN YUNoch keine Bewertungen
- 099 - Small Ruminant HealthDokument49 Seiten099 - Small Ruminant HealthSuraj_Subedi100% (1)
- Title Prevalence of Infections in Residential Care Homes (Rches) For The Elderly in Hong KongDokument39 SeitenTitle Prevalence of Infections in Residential Care Homes (Rches) For The Elderly in Hong KongHam FGNoch keine Bewertungen
- Corona Virus Variants: Sars-Cov - Mers-Cov - CovidDokument25 SeitenCorona Virus Variants: Sars-Cov - Mers-Cov - CovidJenny Agustin FabrosNoch keine Bewertungen
- Susbtratos en MicroDokument17 SeitenSusbtratos en MicroEva SorianoNoch keine Bewertungen
- Immulite: Anti-Hbc IgmDokument28 SeitenImmulite: Anti-Hbc IgmpinoponiNoch keine Bewertungen
- Year 10 DPP Biology Term 3 Exam RevisionDokument8 SeitenYear 10 DPP Biology Term 3 Exam RevisionPoojit VenugopalaNoch keine Bewertungen
- Chapter2 Template Group 1Dokument8 SeitenChapter2 Template Group 1Alessa LamesNoch keine Bewertungen
- Biology of Blood and Marrow TransplantationDokument7 SeitenBiology of Blood and Marrow Transplantationindah sariNoch keine Bewertungen
- Lecture 01 - Introduction To ParasitologyDokument38 SeitenLecture 01 - Introduction To ParasitologyGiorgos Doukas KaranasiosNoch keine Bewertungen
- MCQ Immunology BasicDokument71 SeitenMCQ Immunology BasicMatthew HallNoch keine Bewertungen
- Bourgi 2017Dokument9 SeitenBourgi 2017winter wineNoch keine Bewertungen
- Vaccines: Wim Jiskoot, Gideon F. A. Kersten, Enrico Mastrobattista, and Bram SlütterDokument24 SeitenVaccines: Wim Jiskoot, Gideon F. A. Kersten, Enrico Mastrobattista, and Bram SlütterSaritaJQM100% (1)
- Cepa ATCC 6538Dokument2 SeitenCepa ATCC 6538joshikoNoch keine Bewertungen
- GENERAL BIOLOGY 1 AnswerDokument12 SeitenGENERAL BIOLOGY 1 AnswerKyle DomingoNoch keine Bewertungen
- 0 - Second Wave Covid 19 For Webinar KARS PERSI 24 April 2020 by DickyDokument26 Seiten0 - Second Wave Covid 19 For Webinar KARS PERSI 24 April 2020 by DickyGatot YuliantoNoch keine Bewertungen
- FELASA RodentDokument23 SeitenFELASA RodentprakashgeriyolNoch keine Bewertungen