Das könnte Ihnen auch gefallen
- Clinical Differences Among Four Common Dementia SyndromesDokument2 SeitenClinical Differences Among Four Common Dementia SyndromesIsaac EliasNoch keine Bewertungen
- Music Therapy 1967202930Dokument61 SeitenMusic Therapy 1967202930Auto Grig100% (6)
- Dimentia DiseaseDokument10 SeitenDimentia Diseaseernie16estreraNoch keine Bewertungen
- Alzheimers DiseaseDokument32 SeitenAlzheimers DiseaseBushra EjazNoch keine Bewertungen
- Autism, Psychosis, or Both - Unraveling Complex Patient PresentationsDokument11 SeitenAutism, Psychosis, or Both - Unraveling Complex Patient PresentationsKarina CifuentesNoch keine Bewertungen
- 2783 - 8 - Family Ass ToolsDokument70 Seiten2783 - 8 - Family Ass ToolsFarhry Alvini RahmaniaNoch keine Bewertungen
- Organisational Behavior - NotesDokument21 SeitenOrganisational Behavior - NotesLakshya Tanwar93% (15)
- Alzheimer FinalDokument121 SeitenAlzheimer FinalJoanne Foja100% (1)
- Dementia: Dementia, Also Referred To As Major Neurocognitive Disorder in DSM-5, IsDokument20 SeitenDementia: Dementia, Also Referred To As Major Neurocognitive Disorder in DSM-5, IsTurky DallolNoch keine Bewertungen
- Child Developmental ChecklistDokument4 SeitenChild Developmental ChecklistLindsey NunezNoch keine Bewertungen
- Dementia A Neurodegenerative DisorderDokument16 SeitenDementia A Neurodegenerative DisorderRishabh SinghNoch keine Bewertungen
- Dementia - A Way Ahead: A user-friendly guide for dementia enriched with therapeutic information to assist & empower family & carersVon EverandDementia - A Way Ahead: A user-friendly guide for dementia enriched with therapeutic information to assist & empower family & carersNoch keine Bewertungen
- Vascular DementiaDokument57 SeitenVascular Dementiadrkadiyala2Noch keine Bewertungen
- Annotated BibliographyDokument2 SeitenAnnotated BibliographyJessicaHernandez100% (1)
- 9 Principles of Learning (Assignment)Dokument2 Seiten9 Principles of Learning (Assignment)Arangote Glenn50% (2)
- Alzheimer's Disease Fact SheetDokument6 SeitenAlzheimer's Disease Fact SheetInternational Business Times100% (2)
- Architecture in Theraupetic EnvironmentsDokument27 SeitenArchitecture in Theraupetic EnvironmentsJoshua RevanthNoch keine Bewertungen
- Muscular DystoniaDokument20 SeitenMuscular Dystoniarudresh singhNoch keine Bewertungen
- Degenerative Brain Diseases Impact On How People ActDokument4 SeitenDegenerative Brain Diseases Impact On How People ActSHENNA MAE SADICONNoch keine Bewertungen
- Guarin, Consuelito Danzelle G. PHARM 1-C 0994 Pathophysiology of Nervous SystemDokument9 SeitenGuarin, Consuelito Danzelle G. PHARM 1-C 0994 Pathophysiology of Nervous SystemChelito GuarinNoch keine Bewertungen
- Kolinergik - Alzheimers DiseaseDokument23 SeitenKolinergik - Alzheimers DiseaseCurieThamerNoch keine Bewertungen
- Late Life and Neurocognitive DisordersDokument24 SeitenLate Life and Neurocognitive DisordersJonnaNoch keine Bewertungen
- Refrat Vascular DementiaDokument12 SeitenRefrat Vascular DementiaDebri ErwendiNoch keine Bewertungen
- Neuroregeneration FIX BEUTTDokument61 SeitenNeuroregeneration FIX BEUTTNurcahyo Tri UtomoNoch keine Bewertungen
- Refrat Vascular DementiaDokument13 SeitenRefrat Vascular DementiaAdi AstronNoch keine Bewertungen
- DementiaDokument2 SeitenDementiaGencris Medrano Giray RNNoch keine Bewertungen
- Physiotherapy Rehabilitation For Dementia in Elderly Population. (Abin Abraham Mammen, Sharath Hullumani V, Jakka Rahul)Dokument6 SeitenPhysiotherapy Rehabilitation For Dementia in Elderly Population. (Abin Abraham Mammen, Sharath Hullumani V, Jakka Rahul)ABIN ABRAHAM MAMMEN (PHYSIOTHERAPIST)Noch keine Bewertungen
- Javad Jamshidi MSC of Human Geneticas Shahid Beheshti University of Medical Sciences J.Jamshidi@Sbmu - Ac.IrDokument21 SeitenJavad Jamshidi MSC of Human Geneticas Shahid Beheshti University of Medical Sciences J.Jamshidi@Sbmu - Ac.IrabolojeenNoch keine Bewertungen
- Neurodegenerative Disease 1Dokument6 SeitenNeurodegenerative Disease 1tranthanhnguyen152Noch keine Bewertungen
- Assessment Task-3 (Dementia Disease)Dokument10 SeitenAssessment Task-3 (Dementia Disease)Ashesh BasnetNoch keine Bewertungen
- Gale2018 PDFDokument27 SeitenGale2018 PDFSebastian OrdoñezNoch keine Bewertungen
- Vascular DementiaDokument5 SeitenVascular DementiaAna Ramos LopezNoch keine Bewertungen
- Alzheimer's Disease Information Page - National Institute of Neurological Disorders and StrokeDokument11 SeitenAlzheimer's Disease Information Page - National Institute of Neurological Disorders and StrokeXICMENNoch keine Bewertungen
- Vascular Dementia: Prevention and Treatment: Catherine Mcveigh Peter PassmoreDokument7 SeitenVascular Dementia: Prevention and Treatment: Catherine Mcveigh Peter PassmoreShelia LewisNoch keine Bewertungen
- Thesis Papers Alzheimers DiseaseDokument6 SeitenThesis Papers Alzheimers Diseasehollyschulzgilbert100% (2)
- Alzheimers Research Paper TopicsDokument8 SeitenAlzheimers Research Paper Topicsegyr68dw100% (1)
- Mci, Dementia, Alzheimer DiseaseDokument60 SeitenMci, Dementia, Alzheimer DiseaseDave Siahaan de KaratekaNoch keine Bewertungen
- What Is NeurodegenerationDokument8 SeitenWhat Is NeurodegenerationJuan Castaño CastroNoch keine Bewertungen
- Whatis DementiaDokument3 SeitenWhatis DementiaCamara Cu ZambeteNoch keine Bewertungen
- NIH Public Access: Vascular DementiaDokument23 SeitenNIH Public Access: Vascular DementianadaNoch keine Bewertungen
- Brochure Basicsofalz LowDokument28 SeitenBrochure Basicsofalz LowIbrahim HalilovicNoch keine Bewertungen
- DementiaDokument38 SeitenDementiarajikakurupNoch keine Bewertungen
- Cerebral Atrophy Information Page - National Institute of Neurological Disorders and StrokeDokument3 SeitenCerebral Atrophy Information Page - National Institute of Neurological Disorders and Strokeilham sarifNoch keine Bewertungen
- Alzheimer DiseaseDokument47 SeitenAlzheimer DiseaseveraveroNoch keine Bewertungen
- Normal Aging and Dementia: September 2016Dokument23 SeitenNormal Aging and Dementia: September 2016Adryan RoyNoch keine Bewertungen
- Neuropsychological Contributions To The Early Identification of Alzheimer's DiseaseDokument18 SeitenNeuropsychological Contributions To The Early Identification of Alzheimer's DiseaseLLita LLitolaNoch keine Bewertungen
- Dementia - Definition of Dementia by Medical DictionaryDokument4 SeitenDementia - Definition of Dementia by Medical DictionaryMeryem AfayaNoch keine Bewertungen
- Dementia Vs AlzheimersDokument3 SeitenDementia Vs Alzheimersalfi syahrinNoch keine Bewertungen
- Chap 2 AlzeihmerDokument4 SeitenChap 2 AlzeihmerSabina MoolyeNoch keine Bewertungen
- J Jns 2012 03 027Dokument9 SeitenJ Jns 2012 03 027Juan Jose Eraso OsorioNoch keine Bewertungen
- Multiple Sclerosis Research Paper OutlineDokument6 SeitenMultiple Sclerosis Research Paper Outlinevbbcvwplg100% (1)
- Difference Between Cortical and Subcortical of DementiaDokument7 SeitenDifference Between Cortical and Subcortical of DementiaSanjhanaNoch keine Bewertungen
- Alzheimers InenglishDokument6 SeitenAlzheimers InenglishFrengki PenbainNoch keine Bewertungen
- Cadasil 072007Dokument39 SeitenCadasil 072007doctorebrahimNoch keine Bewertungen
- Discussing The Role of Tau & Amyloid in Alzheimer's (2018)Dokument18 SeitenDiscussing The Role of Tau & Amyloid in Alzheimer's (2018)Brittany JordanNoch keine Bewertungen
- DimentiaDokument5 SeitenDimentiaCristina DodulNoch keine Bewertungen
- Cognition, Mood and Behavior in CADASILDokument6 SeitenCognition, Mood and Behavior in CADASILAna Carolina RibasNoch keine Bewertungen
- Research Paper Alzheimer DiseaseDokument5 SeitenResearch Paper Alzheimer Diseasefzjzn694100% (1)
- The Pathophysiology of Alzheimer'S Disease and Directions in TreatmentDokument15 SeitenThe Pathophysiology of Alzheimer'S Disease and Directions in TreatmentEnerolisa ParedesNoch keine Bewertungen
- D Cognitive Disorders (PR)Dokument111 SeitenD Cognitive Disorders (PR)Japneet KaurNoch keine Bewertungen
- Sample DementiaDokument5 SeitenSample DementiaAlina LazărNoch keine Bewertungen
- Cognitive and Neurologic FunctionDokument38 SeitenCognitive and Neurologic Functioncoosa liquorsNoch keine Bewertungen
- NeurodegenerationDokument8 SeitenNeurodegenerationRommelBaldagoNoch keine Bewertungen
- 05-Normal Physical Changes Nervous SystemDokument23 Seiten05-Normal Physical Changes Nervous Systemsyge zwvuNoch keine Bewertungen
- Polahongon National High School Mahaplag, LeyteDokument7 SeitenPolahongon National High School Mahaplag, LeyteBitoyz Cortes TogononNoch keine Bewertungen
- What Is Alzheimer's Disease?Dokument2 SeitenWhat Is Alzheimer's Disease?JagdishVankarNoch keine Bewertungen
- An Act of ContritionDokument1 SeiteAn Act of ContritionAirene SibleNoch keine Bewertungen
- Agree / Disagree (Opinion Essay) : Typical Question WordsDokument2 SeitenAgree / Disagree (Opinion Essay) : Typical Question WordsAirene SibleNoch keine Bewertungen
- IELTS Advantages and Disadvantages EssayDokument1 SeiteIELTS Advantages and Disadvantages EssayAirene SibleNoch keine Bewertungen
- AugmentinDokument6 SeitenAugmentinAirene SibleNoch keine Bewertungen
- Managing A Disease Is Difficult. Let Us Help. We're Here 24-Hours A Day, 7-Days A Week. 301-588-8200Dokument1 SeiteManaging A Disease Is Difficult. Let Us Help. We're Here 24-Hours A Day, 7-Days A Week. 301-588-8200Airene SibleNoch keine Bewertungen
- Non-Therapeutic CommunicationDokument2 SeitenNon-Therapeutic CommunicationAirene Sible100% (1)
- Coefficient of Thermal Expansion: Contraction EffectsDokument10 SeitenCoefficient of Thermal Expansion: Contraction EffectsAirene SibleNoch keine Bewertungen
- Lesson Title:: Drug EducationDokument3 SeitenLesson Title:: Drug EducationAlyssaNoch keine Bewertungen
- Integration PaperDokument8 SeitenIntegration Paperapi-299783298Noch keine Bewertungen
- Elc Case StudyDokument4 SeitenElc Case Studynazatul shimaNoch keine Bewertungen
- Conclusion and RecommendationDokument1 SeiteConclusion and RecommendationDevorah Jeanne RamosNoch keine Bewertungen
- Research Methods in Life Span Psychology 01062022 122946pm 1 03102022 082731am 18022023 044715pmDokument15 SeitenResearch Methods in Life Span Psychology 01062022 122946pm 1 03102022 082731am 18022023 044715pmaisha ashrafNoch keine Bewertungen
- Harry Stack Sullivan's Interpersonal TheoryDokument1 SeiteHarry Stack Sullivan's Interpersonal TheoryMichal GailNoch keine Bewertungen
- Self EsteemDokument2 SeitenSelf Esteemyesgatl69Noch keine Bewertungen
- Chapter 4Dokument9 SeitenChapter 4dar •Noch keine Bewertungen
- Relationship Between Emotional Intelligence and Psychological Capital With Life Satisfaction in ElderlyDokument8 SeitenRelationship Between Emotional Intelligence and Psychological Capital With Life Satisfaction in ElderlyxbachtiarrNoch keine Bewertungen
- Janina Fisher DISSOCIATIVE PHENOMENA IN THE EVERYDAY LIVES OF TRAUMA SURVIVORSDokument38 SeitenJanina Fisher DISSOCIATIVE PHENOMENA IN THE EVERYDAY LIVES OF TRAUMA SURVIVORSMargaret KelomeesNoch keine Bewertungen
- What Makes Our Life 100 PercentDokument44 SeitenWhat Makes Our Life 100 Percentmail2nsathish100% (2)
- MGT502 Quiz 3 WWW - VustudentsDokument71 SeitenMGT502 Quiz 3 WWW - VustudentsMuddsir Aman33% (3)
- Geriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManDokument12 SeitenGeriatric Nursing: Ma - Alicia Grace S. Kaimo, RN, ManYongNoch keine Bewertungen
- mgt502 10 - MID TERM - SOLVED PAPERDokument143 Seitenmgt502 10 - MID TERM - SOLVED PAPERMuhammad SherjeelNoch keine Bewertungen
- Module Parts Adopting The 5 E's Instructional DesignDokument18 SeitenModule Parts Adopting The 5 E's Instructional DesignSteve GannabanNoch keine Bewertungen
- Malawi Theory of Change Nov2014Dokument15 SeitenMalawi Theory of Change Nov2014priya singhNoch keine Bewertungen
- PARTIALDokument22 SeitenPARTIALJeremiah NoconNoch keine Bewertungen
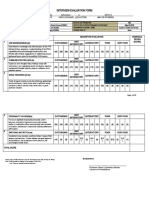
- Annex 3C Interview and Evaluation Form (PCPL To PMSG)Dokument2 SeitenAnnex 3C Interview and Evaluation Form (PCPL To PMSG)JomarNoch keine Bewertungen
- Handouts Career Development ClassDokument26 SeitenHandouts Career Development ClassBillie Balbastre-RoxasNoch keine Bewertungen
- Abnormal Child Psychology 7th Edition Mash Test Bank Full Chapter PDFDokument36 SeitenAbnormal Child Psychology 7th Edition Mash Test Bank Full Chapter PDFKarenMcdonaldedrs100% (15)
- Soc 101 Course OutlineDokument6 SeitenSoc 101 Course OutlineBusayna AlamNoch keine Bewertungen
- Life Insurance Corporation of India: Transformational LeadershipDokument16 SeitenLife Insurance Corporation of India: Transformational LeadershipNilaya Shanker Srivastava100% (1)
- Background To The Functional Dimensions of Coping (FDC) ScaleDokument5 SeitenBackground To The Functional Dimensions of Coping (FDC) Scalejotajota10004950Noch keine Bewertungen