Das könnte Ihnen auch gefallen
- Apex LocatorDokument10 SeitenApex LocatorNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 261 - 264 - The Comparative Sealing Ability of Hydroxyapatite Cement PDFDokument4 Seiten2003 - Journal of Endodontics - 29 - 4 - 261 - 264 - The Comparative Sealing Ability of Hydroxyapatite Cement PDFNamrata SachdevaNoch keine Bewertungen
- 2003 Journal-of-Endodontics 29 4 272 274 Secondary-Hyperparathyroidism-A-Case-Report Loushine 009 PDFDokument3 Seiten2003 Journal-of-Endodontics 29 4 272 274 Secondary-Hyperparathyroidism-A-Case-Report Loushine 009 PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 268 - 271 - Effect of An Intraosseous Injection of Depo Medrol On Pu PDFDokument4 Seiten2003 - Journal of Endodontics - 29 - 4 - 268 - 271 - Effect of An Intraosseous Injection of Depo Medrol On Pu PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 252 - 256 - Three Dimensional Quantitation of Periradicular Bone Des PDFDokument5 Seiten2003 - Journal of Endodontics - 29 - 4 - 252 - 256 - Three Dimensional Quantitation of Periradicular Bone Des PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 259 - 260 - Effectiveness of Stannous Fluoride and Calcium Hydroxide PDFDokument2 Seiten2003 - Journal of Endodontics - 29 - 4 - 259 - 260 - Effectiveness of Stannous Fluoride and Calcium Hydroxide PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 248 - 251 - Effects of NaOCl On Bond Strengths of Resin Cements To R PDFDokument4 Seiten2003 - Journal of Endodontics - 29 - 4 - 248 - 251 - Effects of NaOCl On Bond Strengths of Resin Cements To R PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 233 - 239 - The Effect of Various Concentrations of Sodium Hypochlor PDFDokument7 Seiten2003 - Journal of Endodontics - 29 - 4 - 233 - 239 - The Effect of Various Concentrations of Sodium Hypochlor PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 240 - 243 - Induction of Cyclooxygenase 2 mRNA and Protein Expressio PDFDokument4 Seiten2003 - Journal of Endodontics - 29 - 4 - 240 - 243 - Induction of Cyclooxygenase 2 mRNA and Protein Expressio PDFNamrata SachdevaNoch keine Bewertungen
- 2003 - Journal of Endodontics - 29 - 4 - 244 - 247 - Treponema Socranskii in Primary Endodontic Infections As PDFDokument4 Seiten2003 - Journal of Endodontics - 29 - 4 - 244 - 247 - Treponema Socranskii in Primary Endodontic Infections As PDFNamrata SachdevaNoch keine Bewertungen
- Article4 PDFDokument0 SeitenArticle4 PDFNamrata SachdevaNoch keine Bewertungen
- Article5 PDFDokument0 SeitenArticle5 PDFNamrata SachdevaNoch keine Bewertungen
- Article3 PDFDokument0 SeitenArticle3 PDFNamrata SachdevaNoch keine Bewertungen
- Article2 PDFDokument0 SeitenArticle2 PDFNamrata SachdevaNoch keine Bewertungen
- Article1 PDFDokument0 SeitenArticle1 PDFNamrata SachdevaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Nutrition: Important ConceptsDokument12 SeitenNutrition: Important ConceptshafizaqaiNoch keine Bewertungen
- 5 - Circulation GraysDokument33 Seiten5 - Circulation GraysdrmanojkulNoch keine Bewertungen
- Nose Fracture and Deviated SeptumDokument17 SeitenNose Fracture and Deviated Septummimi2188Noch keine Bewertungen
- ECCO 2 Hemodynamics TestDokument3 SeitenECCO 2 Hemodynamics TestpamoralesNoch keine Bewertungen
- 5937 Understanding Nonverbal Communication Guidebook PDFDokument116 Seiten5937 Understanding Nonverbal Communication Guidebook PDFSalomao RodriguesNoch keine Bewertungen
- Descriptive Text: Report Text About Turtle - Giant Tortoise GalapagosDokument5 SeitenDescriptive Text: Report Text About Turtle - Giant Tortoise GalapagospujayantiriskaNoch keine Bewertungen
- Vitamin KDokument15 SeitenVitamin KTooba Sd100% (2)
- Hachi's PermitDokument1 SeiteHachi's PermitBebelyn AlquizarNoch keine Bewertungen
- Reproduction SystemDokument38 SeitenReproduction SystemNurfatin AdilaNoch keine Bewertungen
- Cheat Sheet 2Dokument2 SeitenCheat Sheet 2oushaNoch keine Bewertungen
- Airway Management 1Dokument17 SeitenAirway Management 1kamel6Noch keine Bewertungen
- VSR PDFDokument12 SeitenVSR PDFDrkrunal badaniNoch keine Bewertungen
- Nipah Virus Infection: ImportanceDokument9 SeitenNipah Virus Infection: ImportanceSivaNoch keine Bewertungen
- CT Mbbs by DR ShamolDokument197 SeitenCT Mbbs by DR ShamolSiva Sandeep Chennimalai50% (2)
- Friesen C4ST Amended Input HC Safety Code 6 - 140 Omitted Studies 224pDokument224 SeitenFriesen C4ST Amended Input HC Safety Code 6 - 140 Omitted Studies 224pSeth BarrettNoch keine Bewertungen
- Asphyxia 2Dokument55 SeitenAsphyxia 2api-19916399100% (1)
- Note GuideDokument2 SeitenNote GuideDemetrius Hobgood0% (1)
- The Physiological Changes of PregnancyDokument16 SeitenThe Physiological Changes of PregnancycchaitukNoch keine Bewertungen
- Great Andamanese Lexicon EnglishDokument65 SeitenGreat Andamanese Lexicon EnglishSai VenkateshNoch keine Bewertungen
- Minnesota State High School LeagueDokument2 SeitenMinnesota State High School Leagueapi-301794844Noch keine Bewertungen
- Breast Care in BreastfeedingDokument11 SeitenBreast Care in BreastfeedingBella Cy LopezNoch keine Bewertungen
- Blake VegliaDokument4 SeitenBlake Vegliaapi-400338931Noch keine Bewertungen
- Talasemia de HB S y Talasemia de HB CDokument10 SeitenTalasemia de HB S y Talasemia de HB CAlejandra NúñezNoch keine Bewertungen
- CiprofloxacinDokument2 SeitenCiprofloxacinNika Joy Cabrera AlarconNoch keine Bewertungen
- Chest RadiographyDokument65 SeitenChest RadiographyMunish Dogra100% (1)
- BSCI 4001 Transcript MidtermDokument4 SeitenBSCI 4001 Transcript MidtermLynell Caraang BarayugaNoch keine Bewertungen
- Follow Site Quarantine ProceduresDokument67 SeitenFollow Site Quarantine ProceduresJohn James100% (3)
- Annotated BibliographyDokument31 SeitenAnnotated BibliographyLara MelissaNoch keine Bewertungen
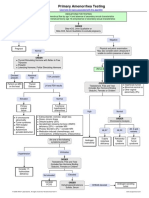
- Primary Amenorrhea Testing AlgorithmDokument1 SeitePrimary Amenorrhea Testing AlgorithmGabriella AguirreNoch keine Bewertungen
- Glossary English - Romanian Medical TermsDokument4 SeitenGlossary English - Romanian Medical TermsGhita Geanina0% (1)