Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Judul Penelit I Alat HasilDokument3 SeitenJudul Penelit I Alat Hasilmanda_jessicaNoch keine Bewertungen
- 7 IdentDokument5 Seiten7 Identmanda_jessicaNoch keine Bewertungen
- Tabel 1Dokument9 SeitenTabel 1manda_jessicaNoch keine Bewertungen
- 3 64 MultisliceDokument11 Seiten3 64 Multislicemanda_jessicaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Media Kit (Viet)Dokument2 SeitenMedia Kit (Viet)Nguyen Ho Thien DuyNoch keine Bewertungen
- HR Recruiter Interview Question & AnswerDokument6 SeitenHR Recruiter Interview Question & AnswerGurukrushna PatnaikNoch keine Bewertungen
- Functions of Communication Oral Communication PDFDokument12 SeitenFunctions of Communication Oral Communication PDFKrystle Francess Barrios0% (1)
- SDLC Review ChecklistDokument4 SeitenSDLC Review Checklistmayank govilNoch keine Bewertungen
- Breathing: Joshua, Youssef, and ApolloDokument28 SeitenBreathing: Joshua, Youssef, and ApolloArvinth Guna SegaranNoch keine Bewertungen
- 208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Dokument55 Seiten208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Nikos AthanasiouNoch keine Bewertungen
- Travel Smart: Assignment 1: Project ProposalDokument14 SeitenTravel Smart: Assignment 1: Project ProposalcattytomeNoch keine Bewertungen
- 5909 East Kaviland AvenueDokument1 Seite5909 East Kaviland Avenueapi-309853346Noch keine Bewertungen
- Individual Assignment: Prepared By: Tigist WoldesenbetDokument12 SeitenIndividual Assignment: Prepared By: Tigist WoldesenbetRobel YacobNoch keine Bewertungen
- Human Resource Planning in Health CareDokument3 SeitenHuman Resource Planning in Health CarevishalbdsNoch keine Bewertungen
- 7 Critical Reading StrategiesDokument1 Seite7 Critical Reading StrategiesWilliam Holt100% (2)
- Sections 3 7Dokument20 SeitenSections 3 7ninalgamaryroseNoch keine Bewertungen
- Of Bones and Buddhas Contemplation of TH PDFDokument215 SeitenOf Bones and Buddhas Contemplation of TH PDFCNoch keine Bewertungen
- Let's Try This: Incident: Thoughts: Feelings: Behavior: Incident: Thoughts: Feelings: BehaviorDokument2 SeitenLet's Try This: Incident: Thoughts: Feelings: Behavior: Incident: Thoughts: Feelings: BehaviorJannet Viacruses LarcenaNoch keine Bewertungen
- K 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Dokument28 SeitenK 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Pradeep JainNoch keine Bewertungen
- Unit 4 Place Value Summative RubricDokument1 SeiteUnit 4 Place Value Summative Rubricapi-169564125Noch keine Bewertungen
- Sample Marketing Plan HondaDokument14 SeitenSample Marketing Plan HondaSaqib AliNoch keine Bewertungen
- Dribssa Beyene Security Sector Reform Paradox Somalia PublishedDokument29 SeitenDribssa Beyene Security Sector Reform Paradox Somalia PublishedNanny KebedeNoch keine Bewertungen
- First Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldDokument25 SeitenFirst Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldAndrea Ibañez73% (11)
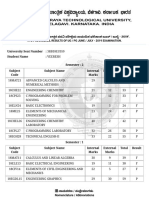
- VTU Result PDFDokument2 SeitenVTU Result PDFVaibhavNoch keine Bewertungen
- How To Write An Argumented EssayDokument35 SeitenHow To Write An Argumented EssayFarhad UllahNoch keine Bewertungen
- Pplied Hysics-Ii: Vayu Education of IndiaDokument16 SeitenPplied Hysics-Ii: Vayu Education of Indiagharib mahmoudNoch keine Bewertungen
- Ryan Brown: Michigan State UniversityDokument2 SeitenRyan Brown: Michigan State UniversitybrownteachesNoch keine Bewertungen
- GEHealthcare Brochure - Discovery CT590 RT PDFDokument12 SeitenGEHealthcare Brochure - Discovery CT590 RT PDFAnonymous ArdclHUONoch keine Bewertungen
- Case StudyDokument3 SeitenCase StudyAnqi Liu50% (2)
- Case Digest: Pedro Elcano and Patricia Elcano Vs - Reginald Hill and Marvin HillDokument5 SeitenCase Digest: Pedro Elcano and Patricia Elcano Vs - Reginald Hill and Marvin Hillshirlyn cuyongNoch keine Bewertungen
- PANIC Origin Story (Part 1)Dokument6 SeitenPANIC Origin Story (Part 1)EpicReads100% (3)
- Cell Bio1Dokument7 SeitenCell Bio1AnyaNoch keine Bewertungen
- Anglicanism QuestionsDokument36 SeitenAnglicanism QuestionsspringsdanielconceptNoch keine Bewertungen
- A Complete List of Greek Underworld GodsDokument3 SeitenA Complete List of Greek Underworld GodsTimothy James M. Madrid100% (1)