Das könnte Ihnen auch gefallen
- How to Write a Dissertation: An Instructional Manual for Dissertation Writers.Von EverandHow to Write a Dissertation: An Instructional Manual for Dissertation Writers.Noch keine Bewertungen
- Literature Review in Research Methodology SlideshareDokument4 SeitenLiterature Review in Research Methodology SlideshareeygyabvkgNoch keine Bewertungen
- RW Reviewer 2nd QTRDokument20 SeitenRW Reviewer 2nd QTRJoshua D.Noch keine Bewertungen
- QRPPDokument19 SeitenQRPPAj Myco EstorNoch keine Bewertungen
- How Long Is A Literature Review DissertationDokument6 SeitenHow Long Is A Literature Review Dissertationafdtsypim100% (1)
- Dissertation Literature Review Example EducationDokument4 SeitenDissertation Literature Review Example EducationqdvtairifNoch keine Bewertungen
- What Is A Literature Review ExamplesDokument8 SeitenWhat Is A Literature Review Examplesea44a6t7100% (1)
- Literature Review Structure ExampleDokument4 SeitenLiterature Review Structure Exampledrnpguwgf100% (1)
- Functions of Review of Related Literature and StudiesDokument7 SeitenFunctions of Review of Related Literature and StudiesafmzubkeaydllzNoch keine Bewertungen
- 3 Parts of A Literature ReviewDokument5 Seiten3 Parts of A Literature Reviewc5e83cmh100% (1)
- Analyzing Research DocumentsDokument8 SeitenAnalyzing Research DocumentsAriel González-CorderoNoch keine Bewertungen
- Writing The Discussion Section of A Literature ReviewDokument7 SeitenWriting The Discussion Section of A Literature ReviewafmzuiffugjdffNoch keine Bewertungen
- How Do You Conclude A Literature ReviewDokument6 SeitenHow Do You Conclude A Literature Reviewaflsnggww100% (1)
- Imrad StyleDokument18 SeitenImrad Styleezradaan0910Noch keine Bewertungen
- Research Paper Vs Literature ReviewDokument6 SeitenResearch Paper Vs Literature Reviewfvey0xan100% (1)
- RESEARCH FRAMEWORKSDokument53 SeitenRESEARCH FRAMEWORKSJhastine Mhae De VeraNoch keine Bewertungen
- Literature Review PartsDokument5 SeitenLiterature Review Partsfrvkuhrif100% (1)
- What Is A Literature Review and What Purpose Does It Serve in The Research ProcessDokument4 SeitenWhat Is A Literature Review and What Purpose Does It Serve in The Research ProcesseygyabvkgNoch keine Bewertungen
- Lecture Nursing ResearchDokument10 SeitenLecture Nursing ResearchAndrea Monique GalasinaoNoch keine Bewertungen
- Difference Between Introduction and Literature Review DissertationDokument8 SeitenDifference Between Introduction and Literature Review DissertationINeedSomeoneToWriteMyPaperSpringfield100% (1)
- What Should Be Included in A Literature ReviewDokument5 SeitenWhat Should Be Included in A Literature Reviewcmppcmwgf100% (1)
- Writing A Literature Review Methods SectionDokument7 SeitenWriting A Literature Review Methods Sectionafmzhfbyasyofd100% (1)
- Which Elements Should A Literature Review Consist ofDokument4 SeitenWhich Elements Should A Literature Review Consist ofjsmyxkvkgNoch keine Bewertungen
- What Is Theoretical Literature Review in ResearchDokument6 SeitenWhat Is Theoretical Literature Review in Researchafdtalblw100% (1)
- Literature Review UefapDokument6 SeitenLiterature Review Uefaptys0v0kan1f3100% (1)
- Wordvice-WPS OfficeDokument7 SeitenWordvice-WPS OfficeMher12Noch keine Bewertungen
- Dissertation Vs Literature ReviewDokument7 SeitenDissertation Vs Literature Reviewc5m8rk4d100% (1)
- Sample Matrix For Literature ReviewDokument7 SeitenSample Matrix For Literature Reviewea84e0rr100% (1)
- DDBA-8005 Conducting A Literature ReviewDokument6 SeitenDDBA-8005 Conducting A Literature ReviewTerry LongNoch keine Bewertungen
- Abstract Vs Literature ReviewDokument5 SeitenAbstract Vs Literature Reviewcmaqqsrif100% (1)
- How To Write A Literature Review For A Dissertation ExampleDokument5 SeitenHow To Write A Literature Review For A Dissertation ExamplenywxluvkgNoch keine Bewertungen
- Literature Review Explains Research ContextDokument7 SeitenLiterature Review Explains Research ContextManohar DhadwadNoch keine Bewertungen
- Hot To Do Literature ReviewDokument4 SeitenHot To Do Literature Reviewgvxphmm8100% (1)
- How To Choose Articles For Literature ReviewDokument4 SeitenHow To Choose Articles For Literature Reviewea86yezd100% (1)
- Purpose of Literature Review in DissertationDokument6 SeitenPurpose of Literature Review in Dissertationea0bvc3s100% (1)
- Difference Between A Literature Review and Research PaperDokument6 SeitenDifference Between A Literature Review and Research PaperafnhgssontbxkdNoch keine Bewertungen
- Objectives of Conducting Literature ReviewDokument10 SeitenObjectives of Conducting Literature Reviewafdtftloi100% (1)
- Steps To Follow in Writing A Literature ReviewDokument7 SeitenSteps To Follow in Writing A Literature Revieweqcusqwgf100% (1)
- To Conduct A Literature ReviewDokument5 SeitenTo Conduct A Literature Reviewc5qz47sm100% (1)
- Literature Review Example Dissertation PDFDokument6 SeitenLiterature Review Example Dissertation PDFafdttjcns100% (1)
- Key Parts of A Literature ReviewDokument5 SeitenKey Parts of A Literature Reviewea6mkqw2100% (1)
- How To Write A Scientific Research Paper - Dr. B.T.LawaniDokument9 SeitenHow To Write A Scientific Research Paper - Dr. B.T.LawaniThe State AcademyNoch keine Bewertungen
- What Is Review of Related Literature in A Research PaperDokument7 SeitenWhat Is Review of Related Literature in A Research PaperaflbtcxfcNoch keine Bewertungen
- Literature Review Sample ShortDokument6 SeitenLiterature Review Sample Shortgw163ckj100% (1)
- Write Literature Review TemplateDokument5 SeitenWrite Literature Review Templateaflsjzblf100% (1)
- What Is A Literature Review in Research MethodsDokument8 SeitenWhat Is A Literature Review in Research Methodsc5rc7ppr100% (1)
- Functions of Review of Related Literature in ResearchDokument8 SeitenFunctions of Review of Related Literature in ResearchgxopkbxgfNoch keine Bewertungen
- Thesis Structure Guidlines enDokument3 SeitenThesis Structure Guidlines enNisreen AwadallahNoch keine Bewertungen
- Chapter 2Dokument16 SeitenChapter 2kasimNoch keine Bewertungen
- Literature Review Example Form 2Dokument7 SeitenLiterature Review Example Form 2afdtuaerl100% (1)
- How To Write A Literature Review For A History DissertationDokument4 SeitenHow To Write A Literature Review For A History DissertationWriteMyCollegePaperForMeCanadaNoch keine Bewertungen
- Literature Review vs. Research ArticleDokument4 SeitenLiterature Review vs. Research Articleafmzwrhwrwohfn100% (1)
- Literature Review Design TypeDokument7 SeitenLiterature Review Design Typefuhukuheseg2100% (1)
- Literature Review Types of ResearchDokument4 SeitenLiterature Review Types of Researcheubvhsvkg100% (1)
- Is A Literature Review Written in Past or Present TenseDokument6 SeitenIs A Literature Review Written in Past or Present TenseafdtszfwbNoch keine Bewertungen
- Reasons For Carrying Out Literature Review in ResearchDokument7 SeitenReasons For Carrying Out Literature Review in Researchc5pgcqzvNoch keine Bewertungen
- Related Literature and Study 1Dokument24 SeitenRelated Literature and Study 1JohnmarvinDalupangDelaCruzNoch keine Bewertungen
- How To Write Literature Review in Master ThesisDokument6 SeitenHow To Write Literature Review in Master Thesisifywpqvcf100% (2)
- Process Literature ReviewDokument7 SeitenProcess Literature Reviewc5qvh6b4100% (1)
- Presentation of Literature Review Lesson Four-1Dokument22 SeitenPresentation of Literature Review Lesson Four-1HudahNoch keine Bewertungen
- PCM PrincipleDokument31 SeitenPCM PrincipleSachin PatelNoch keine Bewertungen
- Average Internal Rate of Return and Investment Decisions: A New PerspectiveDokument40 SeitenAverage Internal Rate of Return and Investment Decisions: A New PerspectiveBharat MaraiyaNoch keine Bewertungen
- Review Questions For COMALGEDokument9 SeitenReview Questions For COMALGEKaye BaguilodNoch keine Bewertungen
- Splunk Quick Reference GuideDokument6 SeitenSplunk Quick Reference GuideLsniperNoch keine Bewertungen
- Role of HypothesisDokument2 SeitenRole of Hypothesisशिवम कर्णNoch keine Bewertungen
- USL - Problem StatementDokument3 SeitenUSL - Problem StatementMarket CharchaNoch keine Bewertungen
- International System of UnitsDokument11 SeitenInternational System of UnitsjbahalkehNoch keine Bewertungen
- POP 301 Production and Operations Management Final ExamDokument2 SeitenPOP 301 Production and Operations Management Final ExamHabib A IslamNoch keine Bewertungen
- Chapter 1ADokument35 SeitenChapter 1ASandip GaikwadNoch keine Bewertungen
- Midterm 3 SolutionsDokument6 SeitenMidterm 3 SolutionscdzavNoch keine Bewertungen
- Fundamentals of Csec Mathematics: Section I Answer All Questions in This Section All Working Must Be Clearly ShownDokument18 SeitenFundamentals of Csec Mathematics: Section I Answer All Questions in This Section All Working Must Be Clearly ShownSamantha JohnsonNoch keine Bewertungen
- Ejercicos Mentales Volumen 13Dokument10 SeitenEjercicos Mentales Volumen 13Luis TorresNoch keine Bewertungen
- ATOA CAE Multiphysics and Multimaterial Design With COMSOL Webinar PDokument31 SeitenATOA CAE Multiphysics and Multimaterial Design With COMSOL Webinar PRaj C ThiagarajanNoch keine Bewertungen
- Engg Mechanics QuestionnaireDokument15 SeitenEngg Mechanics Questionnaireacurvz2005Noch keine Bewertungen
- CV Dr Mohammad ShahzadDokument5 SeitenCV Dr Mohammad ShahzadTarique WaliNoch keine Bewertungen
- Day 2.1 Activity 3 Jemar Wasquin.Dokument5 SeitenDay 2.1 Activity 3 Jemar Wasquin.Jemar WasquinNoch keine Bewertungen
- Risk Management Principles and Guidelines - IsO 31000 ReviewDokument5 SeitenRisk Management Principles and Guidelines - IsO 31000 ReviewMarcelo Coronel Castromonte100% (1)
- The 3-Rainbow Index of GraphsDokument28 SeitenThe 3-Rainbow Index of GraphsDinda KartikaNoch keine Bewertungen
- S Parameter BasicsDokument11 SeitenS Parameter Basicslancelot795Noch keine Bewertungen
- Non Linear Static and Multi Axial Fatigue Analysis of Automotive Lower Control Arm Using NeinastranDokument11 SeitenNon Linear Static and Multi Axial Fatigue Analysis of Automotive Lower Control Arm Using Neinastrangramesh1985Noch keine Bewertungen
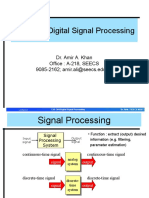
- CSE 304-Digital Signal Processing: Dr. Amir A. Khan Office: A-218, SEECS 9085-2162 Amir - Ali@seecs - Edu.pkDokument22 SeitenCSE 304-Digital Signal Processing: Dr. Amir A. Khan Office: A-218, SEECS 9085-2162 Amir - Ali@seecs - Edu.pkAlamgir Ahmad KhattakNoch keine Bewertungen
- Rr10302 Applied MechanicsDokument12 SeitenRr10302 Applied MechanicsSRINIVASA RAO GANTANoch keine Bewertungen
- Preparation of Vector Group DiffDokument5 SeitenPreparation of Vector Group DiffvenkateshbitraNoch keine Bewertungen
- Solving Problems by Searching: Artificial IntelligenceDokument43 SeitenSolving Problems by Searching: Artificial IntelligenceDai TrongNoch keine Bewertungen
- Maths Parent Workshop Jan 2020Dokument16 SeitenMaths Parent Workshop Jan 2020Marjorie MalvedaNoch keine Bewertungen
- Heat Transfer ME G533 Course OverviewDokument5 SeitenHeat Transfer ME G533 Course OverviewramsastryNoch keine Bewertungen
- Mechanical Vibration NotesDokument56 SeitenMechanical Vibration NotesYadanaNoch keine Bewertungen
- Jyothi Swarup's SAS Programming ResumeDokument4 SeitenJyothi Swarup's SAS Programming Resumethiru_lageshetti368Noch keine Bewertungen
- The Gran Plot 8Dokument5 SeitenThe Gran Plot 8Yasmim YamaguchiNoch keine Bewertungen
- CE6306 NotesDokument125 SeitenCE6306 Noteskl42c4300Noch keine Bewertungen
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)
- The Tennis Partner: A Doctor's Story of Friendship and LossVon EverandThe Tennis Partner: A Doctor's Story of Friendship and LossBewertung: 4.5 von 5 Sternen4.5/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNoch keine Bewertungen
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNoch keine Bewertungen
- Techniques Exercises And Tricks For Memory ImprovementVon EverandTechniques Exercises And Tricks For Memory ImprovementBewertung: 4.5 von 5 Sternen4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Secure Love: Create a Relationship That Lasts a LifetimeVon EverandSecure Love: Create a Relationship That Lasts a LifetimeBewertung: 5 von 5 Sternen5/5 (17)
- The Happiness Trap: How to Stop Struggling and Start LivingVon EverandThe Happiness Trap: How to Stop Struggling and Start LivingBewertung: 4 von 5 Sternen4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- Troubled: A Memoir of Foster Care, Family, and Social ClassVon EverandTroubled: A Memoir of Foster Care, Family, and Social ClassBewertung: 4.5 von 5 Sternen4.5/5 (22)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (327)
- The Ultimate Guide To Memory Improvement TechniquesVon EverandThe Ultimate Guide To Memory Improvement TechniquesBewertung: 5 von 5 Sternen5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisVon EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisBewertung: 5 von 5 Sternen5/5 (3)
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIVon EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIBewertung: 4 von 5 Sternen4/5 (19)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Von EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Bewertung: 5 von 5 Sternen5/5 (1)
- Seeing What Others Don't: The Remarkable Ways We Gain InsightsVon EverandSeeing What Others Don't: The Remarkable Ways We Gain InsightsBewertung: 4 von 5 Sternen4/5 (288)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisVon EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (130)