Das könnte Ihnen auch gefallen
- Conversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresDokument7 SeitenConversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresMaria Von Shaft100% (1)
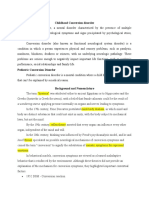
- Childhood Conversion Disorder ExplainedDokument6 SeitenChildhood Conversion Disorder ExplainedFariha Zulfiqar AliNoch keine Bewertungen
- The Essential Handbook of Memory Disorders for CliniciansVon EverandThe Essential Handbook of Memory Disorders for CliniciansNoch keine Bewertungen
- Neuropsychological Evaluation of the Older Adult: A Clinician's GuidebookVon EverandNeuropsychological Evaluation of the Older Adult: A Clinician's GuidebookBewertung: 3 von 5 Sternen3/5 (1)
- Management Of Anger, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandManagement Of Anger, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Neuropsychological Rehabilitation: Principles and ApplicationsVon EverandNeuropsychological Rehabilitation: Principles and ApplicationsJamuna RajeswaranBewertung: 5 von 5 Sternen5/5 (1)
- Lecture Notes in Child and Adolescent PsychiatryVon EverandLecture Notes in Child and Adolescent PsychiatryNoch keine Bewertungen
- Life-Span Developmental Psychology: Research and TheoryVon EverandLife-Span Developmental Psychology: Research and TheoryL. R. GouletBewertung: 3 von 5 Sternen3/5 (1)
- Home Environment and Early Cognitive Development: Longitudinal ResearchVon EverandHome Environment and Early Cognitive Development: Longitudinal ResearchAllen W. GottfriedNoch keine Bewertungen
- Azzam Scale in Practical Guide of Occupational TherapyVon EverandAzzam Scale in Practical Guide of Occupational TherapyNoch keine Bewertungen
- First Aid Tips for Depression: Overcoming Depression In 4 Simple StepsVon EverandFirst Aid Tips for Depression: Overcoming Depression In 4 Simple StepsNoch keine Bewertungen
- Aggression, (Aggressive Behavior) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAggression, (Aggressive Behavior) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Neurodevelopmental Disorders: Comprehensive Developmental NeuroscienceVon EverandNeurodevelopmental Disorders: Comprehensive Developmental NeuroscienceNoch keine Bewertungen
- Detection of Malingering during Head Injury LitigationVon EverandDetection of Malingering during Head Injury LitigationArthur MacNeill Horton, Jr.Noch keine Bewertungen
- Principles and Practice of Child Neurology in Infancy, 2nd EditionVon EverandPrinciples and Practice of Child Neurology in Infancy, 2nd EditionColin KennedyNoch keine Bewertungen
- The Dsm-5 Survival Guide: a Navigational Tool for Mental Health ProfessionalsVon EverandThe Dsm-5 Survival Guide: a Navigational Tool for Mental Health ProfessionalsBewertung: 3 von 5 Sternen3/5 (2)
- A Mind That Found Itself An AutobiographyVon EverandA Mind That Found Itself An AutobiographyBewertung: 5 von 5 Sternen5/5 (1)
- Guilt and ChildrenVon EverandGuilt and ChildrenJane BybeeNoch keine Bewertungen
- Summary of Andrew J. Wakefield's Waging War On The Autistic ChildVon EverandSummary of Andrew J. Wakefield's Waging War On The Autistic ChildNoch keine Bewertungen
- Without Stigma: About the Stigma and the Identity of the Mental IllnessVon EverandWithout Stigma: About the Stigma and the Identity of the Mental IllnessNoch keine Bewertungen
- Meaningful Living across the Lifespan: Occupation-Based Intervention Strategies for Occupational Therapists and ScientistsVon EverandMeaningful Living across the Lifespan: Occupation-Based Intervention Strategies for Occupational Therapists and ScientistsNoch keine Bewertungen
- Foundations of Clinical Psychiatry Fourth EditionVon EverandFoundations of Clinical Psychiatry Fourth EditionBewertung: 5 von 5 Sternen5/5 (1)
- How Verbal Physiotherapy Works, Using Social Delight to Defeat Social Harm, for AllVon EverandHow Verbal Physiotherapy Works, Using Social Delight to Defeat Social Harm, for AllNoch keine Bewertungen
- The Ethics of Psychological ResearchVon EverandThe Ethics of Psychological ResearchJ. D. KeehnNoch keine Bewertungen
- Conversion DisorderDokument48 SeitenConversion Disorderuzma ilyasNoch keine Bewertungen
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementVon EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreNoch keine Bewertungen
- Autism Spectrum Disorder (Updated), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAutism Spectrum Disorder (Updated), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Treatment and Prevention of Alcohol Problems: A Resource ManualVon EverandTreatment and Prevention of Alcohol Problems: A Resource ManualNoch keine Bewertungen
- Neuropsychologist's Journal: Interventions and "Judi-isms"Von EverandNeuropsychologist's Journal: Interventions and "Judi-isms"Noch keine Bewertungen
- The Clinician's Guide to Geriatric Forensic EvaluationsVon EverandThe Clinician's Guide to Geriatric Forensic EvaluationsNoch keine Bewertungen
- New hope for ADHD in children and adults: A practical guideVon EverandNew hope for ADHD in children and adults: A practical guideBewertung: 5 von 5 Sternen5/5 (1)
- Study Guide to Accompany Physiological Psychology Brown/WallaceVon EverandStudy Guide to Accompany Physiological Psychology Brown/WallaceNoch keine Bewertungen
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesVon EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesBewertung: 5 von 5 Sternen5/5 (1)
- Cognition, Brain, and Consciousness: Introduction to Cognitive NeuroscienceVon EverandCognition, Brain, and Consciousness: Introduction to Cognitive NeuroscienceBewertung: 4 von 5 Sternen4/5 (4)
- Schizophrenia: Depression, Hallucinations, Symptoms, and SolutionsVon EverandSchizophrenia: Depression, Hallucinations, Symptoms, and SolutionsNoch keine Bewertungen
- Handbook for the Assessment of Driving CapacityVon EverandHandbook for the Assessment of Driving CapacityMaria T. SchultheisNoch keine Bewertungen
- Diagnostic System: Why the Classification of Psychiatric Disorders Is Necessary, Difficult, and Never SettledVon EverandDiagnostic System: Why the Classification of Psychiatric Disorders Is Necessary, Difficult, and Never SettledNoch keine Bewertungen
- Occupation as the Key to Change: A Collection of Stories and Suggestions Illustrating the Power of OccupationVon EverandOccupation as the Key to Change: A Collection of Stories and Suggestions Illustrating the Power of OccupationNoch keine Bewertungen
- The Role of Emotion and Reflection in Student Achievement: (The Frontal Lobe/ Amygdala Connection)Von EverandThe Role of Emotion and Reflection in Student Achievement: (The Frontal Lobe/ Amygdala Connection)Noch keine Bewertungen
- Brain Injury Rewiring for Loved Ones: A Lifeline to New ConnectionsVon EverandBrain Injury Rewiring for Loved Ones: A Lifeline to New ConnectionsNoch keine Bewertungen
- From Paralysis to Fatigue: A History of Psychosomatic Illness in the Modern EraVon EverandFrom Paralysis to Fatigue: A History of Psychosomatic Illness in the Modern EraBewertung: 5 von 5 Sternen5/5 (1)
- PsychopathologyDokument2 SeitenPsychopathologyMonika JosephNoch keine Bewertungen
- Reflection Paper - BARBA - STEM 101Dokument1 SeiteReflection Paper - BARBA - STEM 101John Miguel BarbaNoch keine Bewertungen
- A Systematic Literature Review of Emotion Regulation Measurement in Individuals With Autism Spectrum DisorderDokument20 SeitenA Systematic Literature Review of Emotion Regulation Measurement in Individuals With Autism Spectrum DisorderKlara BotoNoch keine Bewertungen
- Introduction to Pediatric Nursing Floor Layout and SafetyDokument25 SeitenIntroduction to Pediatric Nursing Floor Layout and SafetyZelel GaliNoch keine Bewertungen
- Behavior and Social SciencesDokument10 SeitenBehavior and Social SciencesRoxana Alexandra BogosNoch keine Bewertungen
- The Perception of The Factors That ContrDokument114 SeitenThe Perception of The Factors That ContrArvind RaveeNoch keine Bewertungen
- Translating The Research Diagnostic Criteria For Temporomandibular Disorders Into Malay: Evaluation of Content and ProcessDokument0 SeitenTranslating The Research Diagnostic Criteria For Temporomandibular Disorders Into Malay: Evaluation of Content and ProcessUniversity Malaya's Dental Sciences ResearchNoch keine Bewertungen
- Padlet Dbsgcog9m7e8Dokument3 SeitenPadlet Dbsgcog9m7e8api-510818103Noch keine Bewertungen
- Introduction to the Major Areas of PsychologyDokument6 SeitenIntroduction to the Major Areas of PsychologyNayyer ShahNoch keine Bewertungen
- Schizophrenia HandbookDokument268 SeitenSchizophrenia HandbookArchana JMNoch keine Bewertungen
- Nihms 446239Dokument9 SeitenNihms 446239Aklile TsegaNoch keine Bewertungen
- Brewin, C. (2014) - Cognitive Foundations of Clinical Psychology PDFDokument229 SeitenBrewin, C. (2014) - Cognitive Foundations of Clinical Psychology PDFMarcela Fernanda Guzmán SánchezNoch keine Bewertungen
- Soc. Sci. 412: Understanding Human BehaviorDokument20 SeitenSoc. Sci. 412: Understanding Human BehaviorClancy HernandezNoch keine Bewertungen
- Blackness and Disability Edited by Christopher BellDokument171 SeitenBlackness and Disability Edited by Christopher BellXian XianNoch keine Bewertungen
- Psychopath Precious MoloiDokument361 SeitenPsychopath Precious MoloiCharlene NyazikaNoch keine Bewertungen
- How To Help Prevent Eating Disorders?Dokument7 SeitenHow To Help Prevent Eating Disorders?Sebastián ValenciaNoch keine Bewertungen
- Social Studies SbaDokument14 SeitenSocial Studies SbaTedesia AssanahNoch keine Bewertungen
- Adverse Childhood Experiences (Aces) : © 2022 Elsevier Ltd. All Rights ReservedDokument16 SeitenAdverse Childhood Experiences (Aces) : © 2022 Elsevier Ltd. All Rights ReservedDiamondChuNoch keine Bewertungen
- Abnormal Psychology Lecture Notes Chapter 1Dokument78 SeitenAbnormal Psychology Lecture Notes Chapter 1che GamboaNoch keine Bewertungen
- Review of Related LiteratureDokument7 SeitenReview of Related LiteratureCj vacaro MendezNoch keine Bewertungen
- Personal Development Diagnostic Test 2022-2023Dokument5 SeitenPersonal Development Diagnostic Test 2022-2023LD 07Noch keine Bewertungen
- Workplace Mental Health and Substance Use Conditions in Male-Dominated Industries: A Systematic Literature ReviewDokument4 SeitenWorkplace Mental Health and Substance Use Conditions in Male-Dominated Industries: A Systematic Literature ReviewMaxNoch keine Bewertungen
- The Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDDokument10 SeitenThe Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDRobi Maulana100% (1)
- Sleep, Recovery, and Human Performance: A Comprehensive Strategy For Long-Term Athlete DevelopmentDokument20 SeitenSleep, Recovery, and Human Performance: A Comprehensive Strategy For Long-Term Athlete DevelopmentSpeed Skating Canada - Patinage de vitesse Canada100% (1)
- Ps TestDokument2 SeitenPs TestAndrada CrimsonNoch keine Bewertungen
- Transdiagnostic TreatmentDokument9 SeitenTransdiagnostic Treatmentvalentina chistrugaNoch keine Bewertungen
- Topics For Presentations - Choose OneDokument13 SeitenTopics For Presentations - Choose OneAnna PratNoch keine Bewertungen
- The Effects of Online Classes On Psychological Health of The Grade 12 Stem StudentsDokument62 SeitenThe Effects of Online Classes On Psychological Health of The Grade 12 Stem StudentsJess Canda100% (4)
- MHLs in IndiaDokument30 SeitenMHLs in IndiaJYOTI100% (1)
- Lecture 20 Concept of Normal and Abnormal BehaviorDokument8 SeitenLecture 20 Concept of Normal and Abnormal BehaviorHariniNoch keine Bewertungen
- PNR Final ExamDokument18 SeitenPNR Final ExaminaderbiNoch keine Bewertungen