Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Notice Tournament August 2018-12Dokument1 SeiteNotice Tournament August 2018-12jitendertalwar1603Noch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Ring GB T 896 1 2Dokument1 SeiteRing GB T 896 1 2jitendertalwar1603Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Notice Tournament August 2018-1Dokument1 SeiteNotice Tournament August 2018-1jitendertalwar1603Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Notice Tournament August 2018-123Dokument1 SeiteNotice Tournament August 2018-123jitendertalwar1603Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- HI& HelloDokument1 SeiteHI& Hellojitendertalwar1603Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data SheetDokument3 Seiten1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data Sheetjitendertalwar1603Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Class Notes Scribd Docs 1 PDFDokument35 SeitenClass Notes Scribd Docs 1 PDFjitendertalwar1603Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Notice Tournament August 2018Dokument1 SeiteNotice Tournament August 2018jitendertalwar1603Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
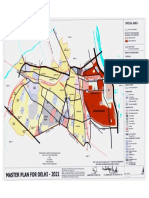
- Special Area Map 2021 Regulations PDFDokument1 SeiteSpecial Area Map 2021 Regulations PDFjitendertalwar1603Noch keine Bewertungen
- 1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data SheetDokument3 Seiten1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data Sheetjitendertalwar1603Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hello PDFDokument15 SeitenHello PDFjitendertalwar1603Noch keine Bewertungen
- Lumax Proposed Circuit Advantages: PCB Design Reduces Cost by 70Dokument1 SeiteLumax Proposed Circuit Advantages: PCB Design Reduces Cost by 70jitendertalwar1603Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hello PDFDokument35 SeitenHello PDFjitendertalwar1603Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- 1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data SheetDokument3 Seiten1 2D Model 2 2 Configuration Se Ings 3: E Ring GB/T 896 1.2 Product Data Sheetjitendertalwar1603Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- 1ring GB T 896 1 2Dokument3 Seiten1ring GB T 896 1 2jitendertalwar1603Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Ring GB T 896 1 2Dokument1 SeiteRing GB T 896 1 2jitendertalwar1603Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Proposal 2 IsoDokument1 SeiteProposal 2 Isojitendertalwar1603Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Ring GB T 896 1 2Dokument1 SeiteRing GB T 896 1 2jitendertalwar1603Noch keine Bewertungen
- Proposal 3-2 IsoDokument1 SeiteProposal 3-2 Isojitendertalwar1603Noch keine Bewertungen
- Proposal 3 IsoDokument1 SeiteProposal 3 Isojitendertalwar1603Noch keine Bewertungen
- Proposal 2 Iso PDFDokument1 SeiteProposal 2 Iso PDFjitendertalwar1603Noch keine Bewertungen
- Proposal 1 IsoDokument1 SeiteProposal 1 Isojitendertalwar1603Noch keine Bewertungen
- Proposal 3 Iso PDFDokument1 SeiteProposal 3 Iso PDFjitendertalwar1603Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- RFQ Details (All Mandatory)Dokument2 SeitenRFQ Details (All Mandatory)jitendertalwar1603Noch keine Bewertungen
- IRCTC e-ticket to Bhopal SHTBDI trainDokument1 SeiteIRCTC e-ticket to Bhopal SHTBDI trainjitendertalwar1603Noch keine Bewertungen
- Furniture DesignDokument26 SeitenFurniture Designparesh09100% (3)
- Ece R010 R4eDokument93 SeitenEce R010 R4ejitendertalwar1603Noch keine Bewertungen
- Blue Ocean Strategy ToolsDokument2 SeitenBlue Ocean Strategy Toolsjitendertalwar1603Noch keine Bewertungen
- Ramshine PVS 701Dokument1 SeiteRamshine PVS 701jitendertalwar1603Noch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)