Das könnte Ihnen auch gefallen
- Cross-Training: The Medical Assistant WorkbookVon EverandCross-Training: The Medical Assistant WorkbookNoch keine Bewertungen
- INZ 1096 - Chest X-Ray Certificate (INZ 1096) - March 2015Dokument8 SeitenINZ 1096 - Chest X-Ray Certificate (INZ 1096) - March 2015Dragoslav DzolicNoch keine Bewertungen
- For Temporary Entry: X-Ray CertificateDokument4 SeitenFor Temporary Entry: X-Ray CertificateJean-Benoît VivequainNoch keine Bewertungen
- General Medical: CertificateDokument16 SeitenGeneral Medical: CertificateMahibul HasanNoch keine Bewertungen
- General Medical: CertificateDokument16 SeitenGeneral Medical: CertificateSheik HassanNoch keine Bewertungen
- INZ 1007 - General Medical Certificate (INZ 1007) March 2015Dokument16 SeitenINZ 1007 - General Medical Certificate (INZ 1007) March 2015Dragoslav Dzolic100% (1)
- General Medical: CertificateDokument16 SeitenGeneral Medical: CertificatethasilvathaNoch keine Bewertungen
- Inz 1007Dokument16 SeitenInz 1007Elijah BoonNoch keine Bewertungen
- Medical and Chest X-Ray CertificateDokument16 SeitenMedical and Chest X-Ray CertificateChristian TonogbanuaNoch keine Bewertungen
- Panel Doctors: Submitting The FormDokument2 SeitenPanel Doctors: Submitting The FormreydudesNoch keine Bewertungen
- Medical Examination For An Australian Visa: CostsDokument9 SeitenMedical Examination For An Australian Visa: CostsApril IngramNoch keine Bewertungen
- Radiological Report On Chest X-Ray of An Applicant For An Australian VisaDokument6 SeitenRadiological Report On Chest X-Ray of An Applicant For An Australian VisaAhmed Fraz MamoonNoch keine Bewertungen
- Health Undertaking: The-Health-Requirement/health-UndertakingsDokument4 SeitenHealth Undertaking: The-Health-Requirement/health-UndertakingsSaadFarazKhanNoch keine Bewertungen
- Immigration New Zealand - 1825063073Dokument3 SeitenImmigration New Zealand - 1825063073Rainers GrīnvaldsNoch keine Bewertungen
- 1 Online AppointmentDokument7 Seiten1 Online AppointmentattitudeNoch keine Bewertungen
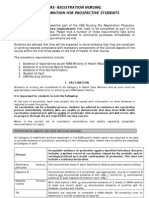
- Application For Registration in New ZealandDokument7 SeitenApplication For Registration in New Zealandjaca lindaNoch keine Bewertungen
- Appendix C: Fill Out This Form and Take It With You To Your Medical AppointmentDokument2 SeitenAppendix C: Fill Out This Form and Take It With You To Your Medical AppointmentJenish MacwanNoch keine Bewertungen
- NG GB enDokument4 SeitenNG GB enahmedakeemNoch keine Bewertungen
- 815Dokument4 Seiten815shantonu_abroad8654Noch keine Bewertungen
- Application To Visit Australia For Medical TreatmentDokument10 SeitenApplication To Visit Australia For Medical TreatmentYvonneSSSNoch keine Bewertungen
- Student Visa Medical Examination FormDokument2 SeitenStudent Visa Medical Examination FormTan Tock Seng HospitalNoch keine Bewertungen
- Migration Health Information Sheet - United Kingdom - Kenya - Clean VersionDokument3 SeitenMigration Health Information Sheet - United Kingdom - Kenya - Clean VersionDerick AbangiNoch keine Bewertungen
- TIA - TiranaDokument14 SeitenTIA - TiranaLaidon ZekajNoch keine Bewertungen
- Step 4: Review Interview GuidelinesDokument8 SeitenStep 4: Review Interview GuidelinesThalía Landeo LozanoNoch keine Bewertungen
- Health Requirement For Temporary Entry To AustraliaDokument2 SeitenHealth Requirement For Temporary Entry To AustraliaBalan PalaniappanNoch keine Bewertungen
- Form 26 PDFDokument0 SeitenForm 26 PDFAnonymous 6tuR1hzNoch keine Bewertungen
- Application For Trans Tasman Mutual Recognition As A Registered Nurse Enrolled Nurse or Midwife ATMR 04Dokument6 SeitenApplication For Trans Tasman Mutual Recognition As A Registered Nurse Enrolled Nurse or Midwife ATMR 04binto111Noch keine Bewertungen
- TIA Tirana 092619Dokument24 SeitenTIA Tirana 092619Maringlen XhaferriNoch keine Bewertungen
- Medical Examination For An Australian Visa: Your ResponsibilitiesDokument10 SeitenMedical Examination For An Australian Visa: Your ResponsibilitiesKapil MehtaNoch keine Bewertungen
- Application To Resume Australian Citizenship: Step 1 - EligibilityDokument15 SeitenApplication To Resume Australian Citizenship: Step 1 - Eligibilityulysses.carvalhoNoch keine Bewertungen
- 737c7e35-8660-424d-bdad-d96cb924e126Dokument4 Seiten737c7e35-8660-424d-bdad-d96cb924e126singhjeet199910Noch keine Bewertungen
- Application For General Registration Graduated or Trained Overseas As A Registered Nurse Enrolled Nurse or Midwife AGOS 40Dokument10 SeitenApplication For General Registration Graduated or Trained Overseas As A Registered Nurse Enrolled Nurse or Midwife AGOS 40karuna26Noch keine Bewertungen
- Medical Examination For An Australian VisaDokument8 SeitenMedical Examination For An Australian VisaamitnshethNoch keine Bewertungen
- AXA PPP Claim Form PDFDokument2 SeitenAXA PPP Claim Form PDFEleftheria AggeleaNoch keine Bewertungen
- Medical Board Form Application Limited Registration For An Area of Need As A Medical Practitioner AANG 30Dokument22 SeitenMedical Board Form Application Limited Registration For An Area of Need As A Medical Practitioner AANG 30Anonymous HA72fUNoch keine Bewertungen
- VisaDokument6 SeitenVisaKNoch keine Bewertungen
- 48 MeDokument15 Seiten48 MeBrajesh Pandey100% (1)
- Registering As A Dentist With The General Dental Council (Overseas Qualified)Dokument18 SeitenRegistering As A Dentist With The General Dental Council (Overseas Qualified)zahra seraj0% (1)
- R13 Czech Slovak Advice SheetDokument5 SeitenR13 Czech Slovak Advice Sheetanon-548408100% (2)
- Laura's DocumentsDokument3 SeitenLaura's DocumentslauraverrellezaNoch keine Bewertungen
- Application To Resume Australian Citizenship: Step 1 - EligibilityDokument16 SeitenApplication To Resume Australian Citizenship: Step 1 - EligibilityPetar KovacevicNoch keine Bewertungen
- Info Sheet - Document Preparation-New Candidates - 2022Dokument1 SeiteInfo Sheet - Document Preparation-New Candidates - 2022Boachie Agyemang-AdolfNoch keine Bewertungen
- APC Three Part Assessment ProcessDokument8 SeitenAPC Three Part Assessment ProcessJacob JonesNoch keine Bewertungen
- Australia Medical Q & A'Dokument5 SeitenAustralia Medical Q & A'Nasir MalikNoch keine Bewertungen
- Nursing and Midwifery Board Form Application For General Registration AGEN 40Dokument12 SeitenNursing and Midwifery Board Form Application For General Registration AGEN 40JinkydelosReyesNoch keine Bewertungen
- Application For Australian Citizenship by Descent: Step 1 - EligibilityDokument13 SeitenApplication For Australian Citizenship by Descent: Step 1 - EligibilityCormac O'KeeffeNoch keine Bewertungen
- Please Read Before Your Appointment: Notice Regarding COVID-19 Infection Prevention MeasuresDokument2 SeitenPlease Read Before Your Appointment: Notice Regarding COVID-19 Infection Prevention MeasuresAii GhieNoch keine Bewertungen
- KuyaDokument2 SeitenKuyaGegeyz1028Noch keine Bewertungen
- Application - Initial Registration: Personal DetailsDokument10 SeitenApplication - Initial Registration: Personal DetailsbronebroneNoch keine Bewertungen
- 866 Application For A Protection (Class XA)Dokument107 Seiten866 Application For A Protection (Class XA)mayootyrNoch keine Bewertungen
- Claim Form en Nov 08Dokument4 SeitenClaim Form en Nov 08Juju FernsNoch keine Bewertungen
- Uktbdp Ghana PDFDokument9 SeitenUktbdp Ghana PDFSqueegee's PalNoch keine Bewertungen
- Renunciation of Citizenship FormDokument11 SeitenRenunciation of Citizenship FormjosephkiwiNoch keine Bewertungen
- U.S. Embassy San Jose, Costa Rica - SNJ 2Dokument1 SeiteU.S. Embassy San Jose, Costa Rica - SNJ 2RaiHernándezNoch keine Bewertungen
- Skills Assessment Application - Without A Skilled Employment Assessment - 1013Dokument9 SeitenSkills Assessment Application - Without A Skilled Employment Assessment - 1013Faisal Inayat AliNoch keine Bewertungen
- OVHC Claim Form 102017 PDFDokument3 SeitenOVHC Claim Form 102017 PDFtarmudiNoch keine Bewertungen
- Pre-Registration Nursing Information For Prospective StudentsDokument4 SeitenPre-Registration Nursing Information For Prospective StudentsbthangarajNoch keine Bewertungen
- Request For Health ExaminationsDokument4 SeitenRequest For Health ExaminationsFaisalNoch keine Bewertungen
- Filter MideaDokument22 SeitenFilter MideaMahibul HasanNoch keine Bewertungen
- Application To Polly Biddut SamityDokument4 SeitenApplication To Polly Biddut SamityMahibul HasanNoch keine Bewertungen
- Application To Polly Biddut SamityDokument1 SeiteApplication To Polly Biddut SamityMahibul HasanNoch keine Bewertungen
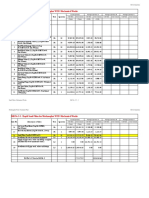
- Consultant Co,. LTD.: Karnaphuli Water Supply Project-Phase 2Dokument1 SeiteConsultant Co,. LTD.: Karnaphuli Water Supply Project-Phase 2Mahibul HasanNoch keine Bewertungen
- Chittagong University of Engineering & Technology: Chittagong - 4349 Course Registration FormDokument1 SeiteChittagong University of Engineering & Technology: Chittagong - 4349 Course Registration FormMahibul HasanNoch keine Bewertungen
- Casting Schedule of May 2016 PDFDokument1 SeiteCasting Schedule of May 2016 PDFMahibul HasanNoch keine Bewertungen
- Construction of Modunaghat Water Treatment Plant & Patenga Booster Pump Station (Cwsisp/W-1)Dokument4 SeitenConstruction of Modunaghat Water Treatment Plant & Patenga Booster Pump Station (Cwsisp/W-1)Mahibul HasanNoch keine Bewertungen
- Strength GainDokument1 SeiteStrength GainMahibul HasanNoch keine Bewertungen
- Schedule - June 2016 PDFDokument2 SeitenSchedule - June 2016 PDFMahibul HasanNoch keine Bewertungen
- Test of Unit Weight (Loose/Roded)Dokument1 SeiteTest of Unit Weight (Loose/Roded)Mahibul HasanNoch keine Bewertungen
- Fin 320 - Individual AssignmentDokument14 SeitenFin 320 - Individual AssignmentAnis Umaira Mohd LutpiNoch keine Bewertungen
- Intern JanataDokument59 SeitenIntern JanataKhairul IslamNoch keine Bewertungen
- ACCA Strategic Business Reporting (SBR) Workbook 2020Dokument840 SeitenACCA Strategic Business Reporting (SBR) Workbook 2020Azba Nishath0% (1)
- (FORD) Manual de Propietario Ford Ranger 1998Dokument160 Seiten(FORD) Manual de Propietario Ford Ranger 1998Marly Salas GonzalezNoch keine Bewertungen
- Marketing Plan Potato Food TruckDokument25 SeitenMarketing Plan Potato Food TruckAhasan h. ShuvoNoch keine Bewertungen
- Bird Beak Adaptations: PurposeDokument9 SeitenBird Beak Adaptations: PurposelilazrbNoch keine Bewertungen
- Student EssaysDokument41 SeitenStudent EssaysAsif RahmanNoch keine Bewertungen
- Nursing ManagementDokument5 SeitenNursing Managementheron_bayanin_15Noch keine Bewertungen
- A Cultura-Mundo - Resposta A Uma SociedDokument7 SeitenA Cultura-Mundo - Resposta A Uma SociedSevero UlissesNoch keine Bewertungen
- IRDM Assignment-I PDFDokument4 SeitenIRDM Assignment-I PDFPiyush AggarwalNoch keine Bewertungen
- A Guide To Energy Efficiency ComplianceDokument16 SeitenA Guide To Energy Efficiency ComplianceOARIASCONoch keine Bewertungen
- SpeechGeek H.I.-larious Volume 3Dokument9 SeitenSpeechGeek H.I.-larious Volume 3SpeechGeekNoch keine Bewertungen
- InflibnetDokument3 SeitenInflibnetSuhotra GuptaNoch keine Bewertungen
- Book2Chapter10 and 11 EvaluationDokument55 SeitenBook2Chapter10 and 11 EvaluationEmmanuel larbiNoch keine Bewertungen
- Jackson R. Lanning: Profile StatementDokument1 SeiteJackson R. Lanning: Profile StatementJacksonLanningNoch keine Bewertungen
- BasicsDokument1 SeiteBasicsRishi Raj100% (1)
- Vibration Absorbers: Scan This QR CodeDokument4 SeitenVibration Absorbers: Scan This QR CodeMohamed RaafatNoch keine Bewertungen
- Hard Rock Tunnelling MethodsDokument20 SeitenHard Rock Tunnelling Methodskiranism0% (1)
- Roundtracer Flash En-Us Final 2021-06-09Dokument106 SeitenRoundtracer Flash En-Us Final 2021-06-09Kawee BoonsuwanNoch keine Bewertungen
- Confirmation 2Dokument11 SeitenConfirmation 2حمزة دراغمةNoch keine Bewertungen
- Marichu Gonzales: Work ExperienceDokument2 SeitenMarichu Gonzales: Work ExperienceMich NavorNoch keine Bewertungen
- Fluid Mechanics and Machinery Laboratory Manual: by Dr. N. Kumara SwamyDokument4 SeitenFluid Mechanics and Machinery Laboratory Manual: by Dr. N. Kumara SwamyMD Mahmudul Hasan Masud100% (1)
- FFL/ A: Tutorial On Reed-Solomon Error Correction CodingDokument144 SeitenFFL/ A: Tutorial On Reed-Solomon Error Correction Codingbatman chamkadarNoch keine Bewertungen
- A Simple and Reliable Submental Intubation.68Dokument4 SeitenA Simple and Reliable Submental Intubation.68Tîrban Pantelimon FlorinNoch keine Bewertungen
- Clostridium BotulinumDokument37 SeitenClostridium Botulinummaria dulceNoch keine Bewertungen
- Chapter 3 Rotation and Revolution NotesDokument12 SeitenChapter 3 Rotation and Revolution NotesMERLIN ANTHONYNoch keine Bewertungen
- Freedom SW 2000 Owners Guide (975-0528!01!01 - Rev-D)Dokument48 SeitenFreedom SW 2000 Owners Guide (975-0528!01!01 - Rev-D)MatthewNoch keine Bewertungen
- 4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsDokument10 Seiten4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsMohammedNoch keine Bewertungen
- Axis Bank - Group 4Dokument34 SeitenAxis Bank - Group 4Deep Ghose DastidarNoch keine Bewertungen
- AM2020-AFP1010 Installation Programming OperatingDokument268 SeitenAM2020-AFP1010 Installation Programming OperatingBaron RicthenNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassVon EverandTroubled: A Memoir of Foster Care, Family, and Social ClassBewertung: 4.5 von 5 Sternen4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)