Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Healing CodesDokument6 SeitenHealing CodesDeepak Satsangi100% (6)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Summary of Diabetes Self Care Activities Measure Results From 7 Studies and A Revised Scale PDFDokument8 SeitenThe Summary of Diabetes Self Care Activities Measure Results From 7 Studies and A Revised Scale PDFDiabetesBhNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Group 4 Case Study On Malignant MelanomaDokument7 SeitenGroup 4 Case Study On Malignant MelanomaLance JardiolinNoch keine Bewertungen
- Specialist Nursing Services For Children and Young People With Diabetes PDFDokument20 SeitenSpecialist Nursing Services For Children and Young People With Diabetes PDFDiabetesBhNoch keine Bewertungen
- Consistent Directions of Effect For Established Type 2 Diabetes Risk Variants Across Populations PDFDokument6 SeitenConsistent Directions of Effect For Established Type 2 Diabetes Risk Variants Across Populations PDFDiabetesBhNoch keine Bewertungen
- Effects of An Intervention by A Diabetes Team in Hospitalized Patients With Diabetes PDFDokument3 SeitenEffects of An Intervention by A Diabetes Team in Hospitalized Patients With Diabetes PDFDiabetesBhNoch keine Bewertungen
- Care of Children and Adolescents With Type 1 DiabetesDokument27 SeitenCare of Children and Adolescents With Type 1 Diabetesapi-3840864Noch keine Bewertungen
- Diabetes Care Practice Nurse Roles Attitudes and Concerns PDFDokument8 SeitenDiabetes Care Practice Nurse Roles Attitudes and Concerns PDFDiabetesBhNoch keine Bewertungen
- Genetic Risk Score Constructed Using 14 Susceptibility Alleles For Type2 DiabetesDokument8 SeitenGenetic Risk Score Constructed Using 14 Susceptibility Alleles For Type2 DiabetesDiabetesBhNoch keine Bewertungen
- New Users of Metformin Are at Low Risk of Incident CancerDokument6 SeitenNew Users of Metformin Are at Low Risk of Incident CancerTomy SaputraNoch keine Bewertungen
- Genotype Prediction of Adult Type 2 Diabetes From Adolescence PDFDokument10 SeitenGenotype Prediction of Adult Type 2 Diabetes From Adolescence PDFDiabetesBhNoch keine Bewertungen
- Type 2 Diabetes in The Young PDFDokument13 SeitenType 2 Diabetes in The Young PDFDiabetesBhNoch keine Bewertungen
- Type 2 Diabetes Mellitus Not Quite Exciting Enough PDFDokument11 SeitenType 2 Diabetes Mellitus Not Quite Exciting Enough PDFDiabetesBhNoch keine Bewertungen
- Control of Glycemia and Cardiovascular Risk Factors in Pts With Type 2 Diabetes in Primary Care PDFDokument6 SeitenControl of Glycemia and Cardiovascular Risk Factors in Pts With Type 2 Diabetes in Primary Care PDFDiabetesBhNoch keine Bewertungen
- Is Cancer Risk Associated With Glycaemic Control PDFDokument2 SeitenIs Cancer Risk Associated With Glycaemic Control PDFDiabetesBhNoch keine Bewertungen
- Analysis of The Type 2 Diabetes Associated Single Nucleotide Polymorphisms in The Genes IRS1 and KCNJ11and PPARG2 in Type 1 Diabetes PDFDokument4 SeitenAnalysis of The Type 2 Diabetes Associated Single Nucleotide Polymorphisms in The Genes IRS1 and KCNJ11and PPARG2 in Type 1 Diabetes PDFDiabetesBhNoch keine Bewertungen
- Association of Type 2 Diabetes Susceptibility Variants With Advanced Prostate Cancer Risk in The Breast and Prostate Cancer Cohort Consortium PDFDokument9 SeitenAssociation of Type 2 Diabetes Susceptibility Variants With Advanced Prostate Cancer Risk in The Breast and Prostate Cancer Cohort Consortium PDFDiabetesBhNoch keine Bewertungen
- Glaucoma Incidence in An Unselected Cohort of Diabetic Pts PDFDokument8 SeitenGlaucoma Incidence in An Unselected Cohort of Diabetic Pts PDFDiabetesBhNoch keine Bewertungen
- (RCSI-MUB) Peer Support For Patients With Type 2 Diabetes 2011Dokument8 Seiten(RCSI-MUB) Peer Support For Patients With Type 2 Diabetes 2011DiabetesBhNoch keine Bewertungen
- Young Onset Type 2 Diabetes Families Are The Major Contributors To Genetic Loci in The Diabetes UK Warren PDFDokument7 SeitenYoung Onset Type 2 Diabetes Families Are The Major Contributors To Genetic Loci in The Diabetes UK Warren PDFDiabetesBhNoch keine Bewertungen
- (RCSI-MUB) Relative Views BMC Public Health 2009Dokument10 Seiten(RCSI-MUB) Relative Views BMC Public Health 2009DiabetesBhNoch keine Bewertungen
- Nonreplication in Genetic Association Studies of Obesity and Diabetes Research PDFDokument4 SeitenNonreplication in Genetic Association Studies of Obesity and Diabetes Research PDFDiabetesBhNoch keine Bewertungen
- IDF Report On Climate Change and DiabetesDokument20 SeitenIDF Report On Climate Change and DiabetesDiabetesBhNoch keine Bewertungen
- (Rcsi-Mub) BMC CAM Use in Bahrain 2010Dokument5 Seiten(Rcsi-Mub) BMC CAM Use in Bahrain 2010DiabetesBhNoch keine Bewertungen
- (RCSI-MUB) Patient Generated FAQsDokument7 Seiten(RCSI-MUB) Patient Generated FAQsDiabetesBhNoch keine Bewertungen
- (RCSI-MUB) Patient Views Family Risk Diabetes Care 2009Dokument3 Seiten(RCSI-MUB) Patient Views Family Risk Diabetes Care 2009DiabetesBhNoch keine Bewertungen
- Impact of Covid 19: By: Vipul PrajapatiDokument10 SeitenImpact of Covid 19: By: Vipul PrajapatiVipul PrajapatoNoch keine Bewertungen
- Jurnal Malaria 2Dokument10 SeitenJurnal Malaria 2Richard KejoraNoch keine Bewertungen
- Osha Training Toolbox Talk:: Biological Hazards - Common Signs and Symptoms of InfectionDokument3 SeitenOsha Training Toolbox Talk:: Biological Hazards - Common Signs and Symptoms of InfectionMuhammad AwaisNoch keine Bewertungen
- Icd 10Dokument3 SeitenIcd 10SriHandaryatiNoch keine Bewertungen
- Foundations in Microbiology: TalaroDokument46 SeitenFoundations in Microbiology: Talaromertx013Noch keine Bewertungen
- Quotes On VaccinesDokument6 SeitenQuotes On VaccinesKris BargerNoch keine Bewertungen
- English Question Formation AssignmentDokument3 SeitenEnglish Question Formation AssignmentTeguh ArdiantoNoch keine Bewertungen
- Parkinson's Disease Epidemiology and Primary SymptomsDokument14 SeitenParkinson's Disease Epidemiology and Primary SymptomsShawn HayleyNoch keine Bewertungen
- Gerd GuidelineDokument5 SeitenGerd GuidelineBenny TrisaktyariNoch keine Bewertungen
- Lact 2Dokument14 SeitenLact 2Playersbattle GroundNoch keine Bewertungen
- Sop Alur Pelayanan Pasien TB Rawat JalandocDokument336 SeitenSop Alur Pelayanan Pasien TB Rawat JalandocRahayu HidayatiNoch keine Bewertungen
- Reseach ProposalDokument8 SeitenReseach Proposaljoyce marie asucanNoch keine Bewertungen
- 47-Article Text-305-1-10-20220731Dokument10 Seiten47-Article Text-305-1-10-20220731alyn30274Noch keine Bewertungen
- Health Assessment of Integument SystemDokument57 SeitenHealth Assessment of Integument SystemkuhakuNoch keine Bewertungen
- Cervical-Cancer AWARENESS REPORTDokument9 SeitenCervical-Cancer AWARENESS REPORTJEEJANoch keine Bewertungen
- 1753-Article Text-39640-3-10-20220815Dokument9 Seiten1753-Article Text-39640-3-10-20220815Inah SaritaNoch keine Bewertungen
- Mod Hiv FinalDokument130 SeitenMod Hiv Finalpb infornon100% (1)
- St. Paul University Dumaguete College of Nursing ISO 9001Dokument6 SeitenSt. Paul University Dumaguete College of Nursing ISO 9001Seth Khalil LardausNoch keine Bewertungen
- Lower Gastrointestinal BleedingDokument1 SeiteLower Gastrointestinal Bleedingmango91286Noch keine Bewertungen
- Skripsi Tanpa Bab PembahasanDokument76 SeitenSkripsi Tanpa Bab PembahasanSeptiara NingsihNoch keine Bewertungen
- Presentation On Incidence and PrevalenceDokument17 SeitenPresentation On Incidence and PrevalenceSUBHNoch keine Bewertungen
- Gastroenterology AscitesDokument2 SeitenGastroenterology AscitesNour SamadNoch keine Bewertungen
- DIABETES MELLITUS - DR Neelakanta KaradkalDokument45 SeitenDIABETES MELLITUS - DR Neelakanta KaradkalNRK A OFFICIALNoch keine Bewertungen
- Nagnječenje Mozga - Mehanizam Nastanka I Značaj: SažetakDokument4 SeitenNagnječenje Mozga - Mehanizam Nastanka I Značaj: SažetakKizicIvanaNoch keine Bewertungen
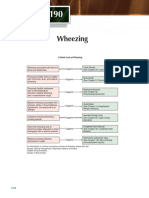
- Chapter 190: A Quick Guide to Wheezing CausesDokument1 SeiteChapter 190: A Quick Guide to Wheezing CausespelinNoch keine Bewertungen
- Iga Afifah Rahmadini 20420020 Intervensi WabahDokument17 SeitenIga Afifah Rahmadini 20420020 Intervensi WabahIga AfifahNoch keine Bewertungen
- DengueDokument4 SeitenDengueNallely LeónNoch keine Bewertungen
- History of St. JudeDokument3 SeitenHistory of St. JudejeezNoch keine Bewertungen