Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mbaeri Accuracy of Prader OrchidometerDokument4 SeitenMbaeri Accuracy of Prader OrchidometerChikezie OnwukweNoch keine Bewertungen
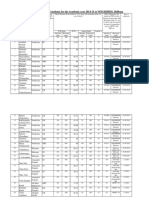
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Dokument10 SeitenAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNoch keine Bewertungen
- Part A Reading Task Playground Injuries Playground Surface MaterialDokument8 SeitenPart A Reading Task Playground Injuries Playground Surface MaterialMitra NabizadehNoch keine Bewertungen
- Understanding Sleep Disorders and Their ClassificationDokument6 SeitenUnderstanding Sleep Disorders and Their ClassificationAh BoonNoch keine Bewertungen
- Above Knee Amputation Exc PDFDokument5 SeitenAbove Knee Amputation Exc PDFSenthilkumar ThiyagarajanNoch keine Bewertungen
- OCPD: Symptoms, Diagnosis and TreatmentDokument4 SeitenOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjNoch keine Bewertungen
- Chapter 9 - Managing Crises and National EmergenciesDokument26 SeitenChapter 9 - Managing Crises and National EmergenciesJayson TasarraNoch keine Bewertungen
- Master Plan for Trivandrum City 2021-2031Dokument21 SeitenMaster Plan for Trivandrum City 2021-2031Adhithy MenonNoch keine Bewertungen
- BG Gluc2Dokument3 SeitenBG Gluc2Nghi NguyenNoch keine Bewertungen
- 100 Days of Jessica Smith Rotation Using DVDsDokument4 Seiten100 Days of Jessica Smith Rotation Using DVDsAusra CrowderNoch keine Bewertungen
- EV3110 SIA Group ReportDokument38 SeitenEV3110 SIA Group ReportWill MyatNoch keine Bewertungen
- Dmaema SDSDokument6 SeitenDmaema SDSToffLinNoch keine Bewertungen
- Research Paper For AbortionDokument10 SeitenResearch Paper For AbortionMarevisha Vidfather75% (4)
- Pediatric Malignant Bone TumoursDokument28 SeitenPediatric Malignant Bone TumourscorneliusNoch keine Bewertungen
- Interactive CME Teaching MethodsDokument5 SeitenInteractive CME Teaching MethodsROMSOPNoch keine Bewertungen
- Sdera Demo Lesson DVD Worksheet 2021Dokument2 SeitenSdera Demo Lesson DVD Worksheet 2021api-396577001Noch keine Bewertungen
- Soap Notes HypertensionDokument6 SeitenSoap Notes HypertensionCHRISTINE KARENDINoch keine Bewertungen
- A Case of Eclectic Family TherapyDokument88 SeitenA Case of Eclectic Family Therapygun gorNoch keine Bewertungen
- PH 021 enDokument4 SeitenPH 021 enjohnllenalcantaraNoch keine Bewertungen
- RPNDokument21 SeitenRPNAruna Teja Chennareddy43% (7)
- Surgery Final NotesDokument81 SeitenSurgery Final NotesDETECTIVE CONANNoch keine Bewertungen
- MudreDokument10 SeitenMudrejezebelvertNoch keine Bewertungen
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDokument7 SeitenPrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalNoch keine Bewertungen
- Pregnancy Calendar For DogsDokument3 SeitenPregnancy Calendar For DogsVina Esther FiguraNoch keine Bewertungen
- SImOS Nano-Tera 2013Dokument35 SeitenSImOS Nano-Tera 2013nanoteraCHNoch keine Bewertungen
- Chemotherapy-Induced Neuropathic PainDokument7 SeitenChemotherapy-Induced Neuropathic Paintita_leo2Noch keine Bewertungen
- 8 Week Shred 1470077297538Dokument2 Seiten8 Week Shred 1470077297538Jesus Castro Machuca0% (1)
- Municipal Ordinance No. 05-2008Dokument5 SeitenMunicipal Ordinance No. 05-2008SBGuinobatan100% (2)
- Occlusion For Implant Suppported CDDokument4 SeitenOcclusion For Implant Suppported CDpopat78Noch keine Bewertungen
- Plant NutrientsDokument10 SeitenPlant NutrientsAdrian GligaNoch keine Bewertungen