Das könnte Ihnen auch gefallen
- Nugzar LipartelianiDokument78 SeitenNugzar LipartelianiTarun SinghNoch keine Bewertungen
- CT 1stDokument60 SeitenCT 1stDrHassan Ahmed ShaikhNoch keine Bewertungen
- CT1 Part 9 Image QualityDokument29 SeitenCT1 Part 9 Image Qualityrazan abdalrhmanNoch keine Bewertungen
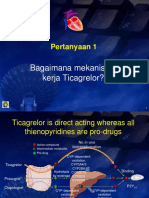
- Pertanyaan ACS TicagrelorDokument5 SeitenPertanyaan ACS TicagrelorwhitecoatNoch keine Bewertungen
- Image EnhancementDokument14 SeitenImage EnhancementsanyamtimeNoch keine Bewertungen
- Lecture 20d CT Image RecontructionDokument40 SeitenLecture 20d CT Image RecontructionLajja Parikh PatelNoch keine Bewertungen
- Tweet TemplateDokument3 SeitenTweet TemplateEutychus2ndNoch keine Bewertungen
- CT Basics - Part 1Dokument27 SeitenCT Basics - Part 1bahadirerNoch keine Bewertungen
- Dynamic Controlled Atmosphere Storage A New Technology For The New York Storage IndustryDokument4 SeitenDynamic Controlled Atmosphere Storage A New Technology For The New York Storage IndustryYogesh KathrechaNoch keine Bewertungen
- Lecture3 Contrast Enhancement PDFDokument46 SeitenLecture3 Contrast Enhancement PDFSahil GandhiNoch keine Bewertungen
- (John C Russ) The Image Processing Cookbook (B-Ok - Xyz)Dokument108 Seiten(John C Russ) The Image Processing Cookbook (B-Ok - Xyz)getinetNoch keine Bewertungen
- 3.RS Image Enhancement 2014Dokument14 Seiten3.RS Image Enhancement 2014Thiwanka Chameera JayasiriNoch keine Bewertungen
- Slide Product Brilinta Crestor AsmihaDokument3 SeitenSlide Product Brilinta Crestor AsmihaMaretha Dyah AnggrainiNoch keine Bewertungen
- Epilepsi PDFDokument11 SeitenEpilepsi PDFJonathan SinartaNoch keine Bewertungen
- Principles of Computer Tomography ImagingDokument331 SeitenPrinciples of Computer Tomography ImagingomarbenhagiNoch keine Bewertungen
- CT Image QualityDokument13 SeitenCT Image QualityRAVI RANJAN- RIMTNoch keine Bewertungen
- CT Image QualityDokument25 SeitenCT Image QualityRa'eel Khan100% (2)
- Imaging of Normal SpineDokument32 SeitenImaging of Normal SpineDestia AnandaNoch keine Bewertungen
- Spinal TuberculosisDokument18 SeitenSpinal TuberculosisKevin KusumanNoch keine Bewertungen
- Pengayaan Koass Ortho - Update 5 VersionDokument122 SeitenPengayaan Koass Ortho - Update 5 Versionanon_967171484Noch keine Bewertungen
- Aktivitas Fisik Pada Dewasa Dan GeriatriDokument20 SeitenAktivitas Fisik Pada Dewasa Dan GeriatriAdinda Suci MaghfiraNoch keine Bewertungen
- Lecture 2// 8.4 CT Numbers, Hounsfield Unit, Gray Scale and Image QualityDokument7 SeitenLecture 2// 8.4 CT Numbers, Hounsfield Unit, Gray Scale and Image QualityThome JerkNoch keine Bewertungen
- Lesson 5 IMAGE QUALITYDokument6 SeitenLesson 5 IMAGE QUALITYWayne De Vergara PalaypayonNoch keine Bewertungen
- Cone Beam Technology: A Brief Technical: History of CAT and CBCTDokument9 SeitenCone Beam Technology: A Brief Technical: History of CAT and CBCTHugo MoralesNoch keine Bewertungen
- Module 1 Computed Tomography and Principles of OperationsDokument6 SeitenModule 1 Computed Tomography and Principles of OperationsWayne De Vergara PalaypayonNoch keine Bewertungen
- Document 39Dokument31 SeitenDocument 392022819384Noch keine Bewertungen
- CT Quality AssuranceDokument9 SeitenCT Quality AssuranceuatilakarathnaNoch keine Bewertungen
- Medical ImagingDokument9 SeitenMedical ImagingRajes WariNoch keine Bewertungen
- Trigger 40 - CTDokument14 SeitenTrigger 40 - CTBriann Louis PaderangaNoch keine Bewertungen
- DI Chap1Dokument9 SeitenDI Chap1HuntingparxxNoch keine Bewertungen
- Ultrasound Image Optimization ("Knobology") - B-ModeDokument12 SeitenUltrasound Image Optimization ("Knobology") - B-ModeSami MoqbelNoch keine Bewertungen
- Currently Available Maxillofacial CBCT EquipmentDokument4 SeitenCurrently Available Maxillofacial CBCT EquipmentzilniNoch keine Bewertungen
- Computed Tomography III: Reconstruction Image Quality ArtifactsDokument33 SeitenComputed Tomography III: Reconstruction Image Quality Artifactsgameplay84Noch keine Bewertungen
- NahidaDokument7 SeitenNahidaانجاز مشاريعNoch keine Bewertungen
- Image Quality and Image ArtifactsDokument22 SeitenImage Quality and Image Artifactslavanyarangaswamy31Noch keine Bewertungen
- BME 404 - Lab08Dokument10 SeitenBME 404 - Lab08abdullah al MamunNoch keine Bewertungen
- Basic Principles of CTDokument77 SeitenBasic Principles of CTcroydubsNoch keine Bewertungen
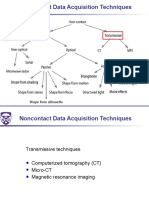
- 08 No Contact Data Asquisition Misc 2019 09 19Dokument47 Seiten08 No Contact Data Asquisition Misc 2019 09 19TimNoch keine Bewertungen
- Characteristics of Multislice CT: Recent TopicsDokument5 SeitenCharacteristics of Multislice CT: Recent TopicsAngelina ProtikNoch keine Bewertungen
- Edited CT Pres GRP 3Dokument37 SeitenEdited CT Pres GRP 3sanyengereNoch keine Bewertungen
- Computed Tomography and Magnetic Resonance ImagingDokument14 SeitenComputed Tomography and Magnetic Resonance ImagingChecko LatteNoch keine Bewertungen
- Welcome To International Journal of Engineering Research and Development (IJERD)Dokument6 SeitenWelcome To International Journal of Engineering Research and Development (IJERD)IJERDNoch keine Bewertungen
- ScanDokument3 SeitenScanLyka SantosNoch keine Bewertungen
- Module 3Dokument7 SeitenModule 3Wayne De Vergara PalaypayonNoch keine Bewertungen
- Geometrik Kedokteran2Dokument5 SeitenGeometrik Kedokteran2tasyaNoch keine Bewertungen
- CT Made ECasyDokument47 SeitenCT Made ECasyAnonymous ceYk4p4Noch keine Bewertungen
- Medical Imaging Systems Example QuestionsDokument2 SeitenMedical Imaging Systems Example QuestionsPika17Noch keine Bewertungen
- Computed Tomography MachineDokument24 SeitenComputed Tomography MachineGaurav Molankar100% (1)
- Cone Beamed Computerized Dental Tomography in DentistryDokument5 SeitenCone Beamed Computerized Dental Tomography in DentistryMeris JugadorNoch keine Bewertungen
- Waldo Tobler 1987Dokument5 SeitenWaldo Tobler 1987jp8c64f9ggNoch keine Bewertungen
- Section 2.3 Spatial Resolution, Pixel Size, and ScaleDokument6 SeitenSection 2.3 Spatial Resolution, Pixel Size, and ScaleShahid AmirNoch keine Bewertungen
- Evaluasi Ketebalan Irisan (Slice Thickness) Pada Pesawat CT-Scan Single SliceDokument7 SeitenEvaluasi Ketebalan Irisan (Slice Thickness) Pada Pesawat CT-Scan Single SliceKyun GazeboNoch keine Bewertungen
- E 1441 - 97 Rte0ndetukveDokument37 SeitenE 1441 - 97 Rte0ndetukveMarceloNoch keine Bewertungen
- Points, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyDokument22 SeitenPoints, Pixels, and Gray Levels: Digitizing Image Data: James B. PawleyÖner AyhanNoch keine Bewertungen
- Volumetric 3D Display For Radiation Therapy PlanningDokument28 SeitenVolumetric 3D Display For Radiation Therapy PlanningNewberryNoch keine Bewertungen
- Computed TomographyDokument4 SeitenComputed TomographyemilyNoch keine Bewertungen
- Module 1 Computed Tomography and Principles of OperationsDokument6 SeitenModule 1 Computed Tomography and Principles of OperationsWayne De Vergara PalaypayonNoch keine Bewertungen
- Segmentation and Feature Extraction LolDokument2 SeitenSegmentation and Feature Extraction LolMansi KasarNoch keine Bewertungen
- CT ScanningDokument24 SeitenCT ScanningMurary S PottyNoch keine Bewertungen
- Intramuscular Injection GuidelinesDokument2 SeitenIntramuscular Injection GuidelinesMehabooba Mehataf100% (1)
- Penguin Restaurant Infront of Cancer HospitalDokument2 SeitenPenguin Restaurant Infront of Cancer HospitalbbkanilNoch keine Bewertungen
- Kei10344 FMDokument4 SeitenKei10344 FMbbkanilNoch keine Bewertungen
- FS41 p34 Aptip Body OncologyDokument5 SeitenFS41 p34 Aptip Body OncologybbkanilNoch keine Bewertungen
- Important Information About Your StatementDokument1 SeiteImportant Information About Your StatementbbkanilNoch keine Bewertungen
- Chapter 4 Scintillation Detectors: 4.1. Basic Principle of The ScintillatorDokument10 SeitenChapter 4 Scintillation Detectors: 4.1. Basic Principle of The ScintillatorbbkanilNoch keine Bewertungen
- Bushong ReviewDokument10 SeitenBushong ReviewbbkanilNoch keine Bewertungen
- Bushong: Radiologic Science For Technologists, 10th EditionDokument6 SeitenBushong: Radiologic Science For Technologists, 10th EditionbbkanilNoch keine Bewertungen
- Bushong Rad ProtectionDokument7 SeitenBushong Rad ProtectionbbkanilNoch keine Bewertungen
- X-Ray Tube DiagramDokument1 SeiteX-Ray Tube DiagrambbkanilNoch keine Bewertungen
- Bipolar Disorder or ManicDokument16 SeitenBipolar Disorder or Manicbbkanil100% (1)
- AAPM Report 39 - CT Acceptance Testing (1993)Dokument101 SeitenAAPM Report 39 - CT Acceptance Testing (1993)DethsorNoch keine Bewertungen
- Prosthetics Lower Limb Catalogue 2012Dokument292 SeitenProsthetics Lower Limb Catalogue 2012mihaela_moldova9128Noch keine Bewertungen
- Multimode Optical Fiber Based SpectrometersDokument16 SeitenMultimode Optical Fiber Based Spectrometersebn123Noch keine Bewertungen
- Strategies For Film Replacement in RadiographyDokument15 SeitenStrategies For Film Replacement in Radiographysaleemut3100% (1)
- En c1316 Sarix Ti Ip ps041311Dokument4 SeitenEn c1316 Sarix Ti Ip ps041311Antonio ChipanaNoch keine Bewertungen
- Week 7 B Chapter 29, 30 Computed Tomography 45Dokument45 SeitenWeek 7 B Chapter 29, 30 Computed Tomography 45freedy freedyNoch keine Bewertungen
- 5.basic SensitometryDokument14 Seiten5.basic SensitometryankamgudeNoch keine Bewertungen
- Full Download Digital Radiography and Pacs 2nd Edition Carter Test BankDokument35 SeitenFull Download Digital Radiography and Pacs 2nd Edition Carter Test Bankbridieditch100% (27)
- Inside ProlithDokument179 SeitenInside ProlithgoucloudNoch keine Bewertungen
- SilverFast Resolution Target (USAF 1951) PDFDokument10 SeitenSilverFast Resolution Target (USAF 1951) PDFsage.electconNoch keine Bewertungen
- Radiamatic II Spec enDokument6 SeitenRadiamatic II Spec enAndrey ClavijoNoch keine Bewertungen
- 2022 @dentolib Antigoni Delantoni, Kaan Orhan Atlas of DentomaxillofacialDokument229 Seiten2022 @dentolib Antigoni Delantoni, Kaan Orhan Atlas of Dentomaxillofacialc8dqt289hfNoch keine Bewertungen
- 04main Measure Insp SensorsDokument66 Seiten04main Measure Insp SensorsJoao RobertoNoch keine Bewertungen
- 2018 OceanOptics InnovationBrochureDokument16 Seiten2018 OceanOptics InnovationBrochureDicky ArintaNoch keine Bewertungen
- RPT 29Dokument79 SeitenRPT 29Vidya NaikNoch keine Bewertungen
- Nano 5Dokument18 SeitenNano 5caralbmarbat_3207679Noch keine Bewertungen
- RDT 112 Prelim SummaryDokument26 SeitenRDT 112 Prelim SummaryJian SolimanNoch keine Bewertungen
- Paper 37472 Manuscript 12431 0 Final UpdatedDokument9 SeitenPaper 37472 Manuscript 12431 0 Final UpdatedAli ArdeshiriNoch keine Bewertungen
- A Beginner's Guide To Ultrasound BiomicrosDokument9 SeitenA Beginner's Guide To Ultrasound BiomicrosSALAH YOUNISNoch keine Bewertungen
- A Low-Cost High-Performance Digital Radar Test BedDokument9 SeitenA Low-Cost High-Performance Digital Radar Test BedWesley ChenNoch keine Bewertungen
- Bangladesh University of Engineering and Technology (Buet), DhakaDokument46 SeitenBangladesh University of Engineering and Technology (Buet), DhakaRashedKhanNoch keine Bewertungen
- Talysurf Cci 6000Dokument3 SeitenTalysurf Cci 6000Parveen SwamiNoch keine Bewertungen
- VersaDoc MP 4000 Sole Source SpecificationsDokument3 SeitenVersaDoc MP 4000 Sole Source SpecificationsdnajenNoch keine Bewertungen
- Checker 4G7C DatasheetDokument3 SeitenChecker 4G7C DatasheetGregg JamesNoch keine Bewertungen
- PikselDokument11 SeitenPikselNur RahmaNoch keine Bewertungen
- Tem PrimerDokument31 SeitenTem Primerjackactforever4Noch keine Bewertungen
- Physics PDFDokument47 SeitenPhysics PDFstoicea_katalinNoch keine Bewertungen
- Diopter Focus of ANVIS EyepiecesDokument39 SeitenDiopter Focus of ANVIS Eyepieceswildan mullerNoch keine Bewertungen
- Missile Approach Warning Systems - The Infrared vs. Ultraviolet Debate Geoff Van HeesDokument14 SeitenMissile Approach Warning Systems - The Infrared vs. Ultraviolet Debate Geoff Van Heessreeramk1350% (2)
- Basic Principles of UltrasoundDokument38 SeitenBasic Principles of UltrasoundredaradeNoch keine Bewertungen