Das könnte Ihnen auch gefallen
- Herbal Formulation Considerations For Autoimmune DisordersDokument26 SeitenHerbal Formulation Considerations For Autoimmune Disordershitesh mendirattaNoch keine Bewertungen
- Banton BiomechanicsDokument9 SeitenBanton BiomechanicsIoan AndraNoch keine Bewertungen
- Surgical Anatomy of NeckDokument37 SeitenSurgical Anatomy of Neckaishwarya raviNoch keine Bewertungen
- Cracking Chests: How Thoracic Surgery Got from Rocks to SticksVon EverandCracking Chests: How Thoracic Surgery Got from Rocks to SticksNoch keine Bewertungen
- M1 All ProgramsDokument26 SeitenM1 All ProgramsDaisy Joy MBardz100% (1)
- High-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsDokument41 SeitenHigh-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsAlvin JulianNoch keine Bewertungen
- BranchialCleftCyst GerDokument36 SeitenBranchialCleftCyst GerDrsreeram Valluri100% (1)
- Review of Internal HerniasDokument15 SeitenReview of Internal HerniassavingtaviaNoch keine Bewertungen
- Thyroid GlandDokument81 SeitenThyroid Glanddr_shamimrNoch keine Bewertungen
- Brain ImagingDokument56 SeitenBrain ImagingAnant PachisiaNoch keine Bewertungen
- Artefactos en Ultrasonido, Un TutorialDokument25 SeitenArtefactos en Ultrasonido, Un Tutorialramon100% (2)
- Radiology SpottersDokument24 SeitenRadiology SpottersSameer VermaNoch keine Bewertungen
- Principals of Cranial Surgery For Tumors MCQ-1Dokument9 SeitenPrincipals of Cranial Surgery For Tumors MCQ-1lonsilord17100% (1)
- Neck Fascia Prof Talib Jawad PDFDokument14 SeitenNeck Fascia Prof Talib Jawad PDFMohamed Farouk El-FaresyNoch keine Bewertungen
- Pedi HN SlidesDokument71 SeitenPedi HN SlidesvelangniNoch keine Bewertungen
- RADIOLOGY 1.7 Neuroradiology (CT)Dokument7 SeitenRADIOLOGY 1.7 Neuroradiology (CT)ZazaNoch keine Bewertungen
- Lecture 1 Historical Aspects of Surgery (Core)Dokument27 SeitenLecture 1 Historical Aspects of Surgery (Core)Charwinth KankaNoch keine Bewertungen
- Aortic DissectionDokument59 SeitenAortic DissectionDwi Gunawan Fardhani100% (1)
- Neurosurgery - Medicine Simplified (DBMCI)Dokument5 SeitenNeurosurgery - Medicine Simplified (DBMCI)pvsvrNoch keine Bewertungen
- Ultrasound Guided Interventional Procedures In.13Dokument14 SeitenUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- DR Parkha RehmanDokument50 SeitenDR Parkha Rehmanmustafa sajjadNoch keine Bewertungen
- Abg AnalysisDokument26 SeitenAbg Analysissridhar100% (11)
- Final Online Exam Guideline CBTDokument105 SeitenFinal Online Exam Guideline CBTfaisalaminwani121Noch keine Bewertungen
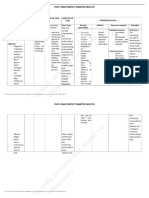
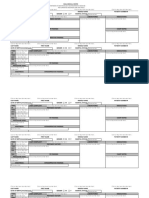
- This Study Resource Was Shared Via: Fncp-Health Deficit: Diabetes MellitusDokument3 SeitenThis Study Resource Was Shared Via: Fncp-Health Deficit: Diabetes MellitusAlhadzra AlihNoch keine Bewertungen
- Blood Can Be Very BadDokument37 SeitenBlood Can Be Very BadPhil SingerNoch keine Bewertungen
- ILAE Classification of Seizures and EpilepsyDokument19 SeitenILAE Classification of Seizures and EpilepsyIRENA GENI100% (1)
- Physics of UltrasoundDokument4 SeitenPhysics of Ultrasound{Phantom}100% (1)
- Ceasarean Case StudyDokument26 SeitenCeasarean Case StudyNarissa Jay Taub YlananNoch keine Bewertungen
- History of Operating RoomDokument9 SeitenHistory of Operating RoomKhrizlynne SoberanoNoch keine Bewertungen
- Cranial Ultrasound: DR Muhammad Jazib ShahidDokument43 SeitenCranial Ultrasound: DR Muhammad Jazib ShahidJazib ShahidNoch keine Bewertungen
- FOUR Score Instruction Guide For Application On MISH ICUDokument2 SeitenFOUR Score Instruction Guide For Application On MISH ICUMohamed Farouk El-FaresyNoch keine Bewertungen
- US OB Review (#1 - 61)Dokument205 SeitenUS OB Review (#1 - 61)Júlio Muniz100% (1)
- Gray's Anatomy Review - Back QuestionsDokument39 SeitenGray's Anatomy Review - Back Questionsandrea100% (2)
- Cardiovascular MCQsDokument23 SeitenCardiovascular MCQssb medexNoch keine Bewertungen
- Sectional AnatomyDokument28 SeitenSectional AnatomyHanadi AbNoch keine Bewertungen
- The New Clasification ILAE 2017Dokument6 SeitenThe New Clasification ILAE 2017Ami D ALNoch keine Bewertungen
- Giovanni Maciocia Menorrhagia NotesDokument22 SeitenGiovanni Maciocia Menorrhagia Noteshihi12100% (5)
- Head and Neck Division Radiology Department Faculty of Medicine University of Indonesia / Cipto Mangunkusumo HospitalDokument65 SeitenHead and Neck Division Radiology Department Faculty of Medicine University of Indonesia / Cipto Mangunkusumo HospitalGinsha Audia Kusumo100% (1)
- Imaging of Orbita and Ear FKDokument70 SeitenImaging of Orbita and Ear FKAprilia Anggela100% (1)
- LincosamidesDokument19 SeitenLincosamidesManahil RiazNoch keine Bewertungen
- Ocular Trauma - BantaDokument211 SeitenOcular Trauma - BantaLuisa Fernanda Arboleda100% (1)
- Lung Pancoast Tumor - StatPearls - NCBI BookshelfDokument9 SeitenLung Pancoast Tumor - StatPearls - NCBI BookshelfAmaliaNoch keine Bewertungen
- Arachnoid CystDokument4 SeitenArachnoid CystSlaviša KovačevićNoch keine Bewertungen
- CT PerfusionDokument6 SeitenCT PerfusionChristopher Whitley100% (1)
- Stroke RadiopaediaDokument3 SeitenStroke RadiopaediaDaniel DumaNoch keine Bewertungen
- UltrasoundDokument20 SeitenUltrasoundyechale tafereNoch keine Bewertungen
- Petrous ApexDokument6 SeitenPetrous ApexSarat Kumar ChalasaniNoch keine Bewertungen
- Wa0030Dokument13 SeitenWa0030lonsilord17Noch keine Bewertungen
- Intradural Extramedullary TumorsDokument10 SeitenIntradural Extramedullary TumorsFaizyab AhmedNoch keine Bewertungen
- MeningesDokument25 SeitenMeningesAsad OsmanNoch keine Bewertungen
- Dance - Davis Intubated Ureterotomy in A Child - 05202016Dokument27 SeitenDance - Davis Intubated Ureterotomy in A Child - 05202016sirrfsNoch keine Bewertungen
- Final Exam National Board of Examinations JUNE 2020Dokument2 SeitenFinal Exam National Board of Examinations JUNE 2020narasimhahanNoch keine Bewertungen
- Benign and Malignant Neoplasia of URTDokument48 SeitenBenign and Malignant Neoplasia of URTsahirbuleNoch keine Bewertungen
- Breast - Dr. HammouriDokument12 SeitenBreast - Dr. HammouriMohammad PropensityNoch keine Bewertungen
- Disorders of Diverticulation and Cleavage, Sulcation andDokument48 SeitenDisorders of Diverticulation and Cleavage, Sulcation andagoyal_9Noch keine Bewertungen
- MediastiniumDokument25 SeitenMediastiniumahmedzakaria0Noch keine Bewertungen
- Superior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014Dokument35 SeitenSuperior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014jhk0428Noch keine Bewertungen
- DR Kaushal Cerebral Blood FlowDokument52 SeitenDR Kaushal Cerebral Blood Flowoddie333Noch keine Bewertungen
- Congenital Cystic Masses of The NeckDokument48 SeitenCongenital Cystic Masses of The NeckEsraa El ShemeNoch keine Bewertungen
- MCQ Sample QuestionsDokument4 SeitenMCQ Sample QuestionsNaveen Vachipalli100% (1)
- Экзам.тесты ИГ 4курс ЛОРDokument98 SeitenЭкзам.тесты ИГ 4курс ЛОРканизаNoch keine Bewertungen
- Vascular Disorders StudentsDokument70 SeitenVascular Disorders StudentsedwinNoch keine Bewertungen
- C 1+ 2 Surgicl Pathology of OesophagusDokument91 SeitenC 1+ 2 Surgicl Pathology of OesophagusSayuridark5Noch keine Bewertungen
- @MedicalBooksStore 2007 Self AssessmentDokument289 Seiten@MedicalBooksStore 2007 Self AssessmentOkka Soe OoNoch keine Bewertungen
- Diaphragmatic ParalysisDokument32 SeitenDiaphragmatic ParalysisSwapnil MehtaNoch keine Bewertungen
- Neurosurgical Emergencies NeuroupdateDokument29 SeitenNeurosurgical Emergencies NeuroupdateAdi SulistyantoNoch keine Bewertungen
- FCPS Part1 Recall Ent Sep 2018Dokument6 SeitenFCPS Part1 Recall Ent Sep 2018rizwan afzalNoch keine Bewertungen
- Neck TrianglesDokument6 SeitenNeck TrianglesJay-arh SebusaNoch keine Bewertungen
- Edited. Ashkar - L's MacBook ProDokument40 SeitenEdited. Ashkar - L's MacBook ProDoina CneagnitchiNoch keine Bewertungen
- The Validity of Multimodal Intraoperative Monitoring (MIOM) in Surgery of 109 Spine and Spinal Cord TumorsDokument12 SeitenThe Validity of Multimodal Intraoperative Monitoring (MIOM) in Surgery of 109 Spine and Spinal Cord TumorsMohamed Farouk El-FaresyNoch keine Bewertungen
- Spinal Trauma: Causes of Cervical Spinal Injury (UK)Dokument16 SeitenSpinal Trauma: Causes of Cervical Spinal Injury (UK)Mohamed Farouk El-FaresyNoch keine Bewertungen
- Suspected Spine TraumaDokument23 SeitenSuspected Spine TraumaMohamed Farouk El-FaresyNoch keine Bewertungen
- Normal Cortical AnatomyDokument49 SeitenNormal Cortical AnatomyMohamed Farouk El-FaresyNoch keine Bewertungen
- Cervical Spine Clearance 2009Dokument7 SeitenCervical Spine Clearance 2009Abdulelah Al.luhaybiNoch keine Bewertungen
- Foreword 2009 NeuromodulationDokument1 SeiteForeword 2009 NeuromodulationMohamed Farouk El-FaresyNoch keine Bewertungen
- Initial Endoscopic Management of Pineal Region Tumors and Associated Hydrocephalus Clinical Series and Literature ReviewDokument5 SeitenInitial Endoscopic Management of Pineal Region Tumors and Associated Hydrocephalus Clinical Series and Literature ReviewMohamed Farouk El-FaresyNoch keine Bewertungen
- Endoscopic Third VentriculostomyDokument4 SeitenEndoscopic Third VentriculostomyMohamed Farouk El-FaresyNoch keine Bewertungen
- A Guide To Placement of Parietooccipital Ventricular CathetersDokument5 SeitenA Guide To Placement of Parietooccipital Ventricular CathetersMohamed Farouk El-FaresyNoch keine Bewertungen
- Pain Assessment ScalesDokument9 SeitenPain Assessment ScalesElham AlsamahiNoch keine Bewertungen
- Graded Chronic Pain ScaleDokument2 SeitenGraded Chronic Pain ScaleMohamed Farouk El-Faresy0% (1)
- Ventricular Volume Following Third VentriculostomyDokument6 SeitenVentricular Volume Following Third VentriculostomyMohamed Farouk El-FaresyNoch keine Bewertungen
- Surgical Approaches To Posterior Third Ventricular TumorsDokument19 SeitenSurgical Approaches To Posterior Third Ventricular TumorsMohamed Farouk El-FaresyNoch keine Bewertungen
- Lack of Benefit of Endoscopic Ventriculoperitoneal Shunt InsertionDokument7 SeitenLack of Benefit of Endoscopic Ventriculoperitoneal Shunt InsertionMohamed Farouk El-FaresyNoch keine Bewertungen
- Endoscopic ApproachDokument13 SeitenEndoscopic ApproachMohamed Farouk El-FaresyNoch keine Bewertungen
- Neuroendoscopy Past Present and FutureDokument5 SeitenNeuroendoscopy Past Present and FutureMohamed Farouk El-FaresyNoch keine Bewertungen
- Cyst 2005 19 6 8Dokument9 SeitenCyst 2005 19 6 8Mohamed Farouk El-FaresyNoch keine Bewertungen
- Intracranial EndosDokument22 SeitenIntracranial EndosMohamed Farouk El-FaresyNoch keine Bewertungen
- The Clinical Significance of The Retromolar Canal and Foramen in DentistryDokument24 SeitenThe Clinical Significance of The Retromolar Canal and Foramen in Dentistryمحمد عبدالرحمنNoch keine Bewertungen
- Full Download Book Medical Epigenetics PDFDokument41 SeitenFull Download Book Medical Epigenetics PDFandrew.lindsey981100% (14)
- Quisted en P Menopausicas Guias GTG - 34 PDFDokument32 SeitenQuisted en P Menopausicas Guias GTG - 34 PDFAdela Marìa P LNoch keine Bewertungen
- UrosepsaDokument2 SeitenUrosepsaHazir AziriNoch keine Bewertungen
- Banerjee 2017Dokument8 SeitenBanerjee 2017FFDFNoch keine Bewertungen
- Tanda, Ciri-Ciri Dan Perbedaan Versi B InggrisDokument2 SeitenTanda, Ciri-Ciri Dan Perbedaan Versi B Inggriselama natilaNoch keine Bewertungen
- Hemato OnologyDokument60 SeitenHemato OnologyGousayAlkhazmariNoch keine Bewertungen
- Gender M F Marital Status: Rizal Medical CenterDokument21 SeitenGender M F Marital Status: Rizal Medical CentermaKitten08Noch keine Bewertungen
- Literature ReviewDokument8 SeitenLiterature Reviewapi-550033018Noch keine Bewertungen
- Journal of Chronic PainDokument8 SeitenJournal of Chronic PainRirin TriyaniNoch keine Bewertungen
- SymbicortDokument18 SeitenSymbicortkaditasookdeoNoch keine Bewertungen
- Thrombolytic Therapy in Acute Myocardial InfarctionDokument7 SeitenThrombolytic Therapy in Acute Myocardial InfarctionRumela Ganguly ChakrabortyNoch keine Bewertungen
- La Union Arrival Card - V1 PDFDokument2 SeitenLa Union Arrival Card - V1 PDFLorei LeeNoch keine Bewertungen
- Tonsillitis, Tonsillectomy and Adenoidectomy: - Literature ReadingDokument52 SeitenTonsillitis, Tonsillectomy and Adenoidectomy: - Literature ReadingdestiNoch keine Bewertungen
- Acute Ischemic StrokeDokument9 SeitenAcute Ischemic Strokepuskesmas tarikNoch keine Bewertungen
- Pancreatic Hormones and Anti Diabetic Drugs NotesDokument8 SeitenPancreatic Hormones and Anti Diabetic Drugs NotesBrunette CesaNoch keine Bewertungen
- Applied Pharmacology For The Dental Hygienist 7th Edition Haveles Solutions ManualDokument24 SeitenApplied Pharmacology For The Dental Hygienist 7th Edition Haveles Solutions ManualJosephCraiggmax100% (50)
- POPS PretestDokument6 SeitenPOPS Pretestkingjameson1Noch keine Bewertungen
- CRRT Cu CitratDokument35 SeitenCRRT Cu CitratAndreea MitranNoch keine Bewertungen
- MS2 - Neurologic Disorder My ReportDokument30 SeitenMS2 - Neurologic Disorder My ReportNeil Lansang BallobanNoch keine Bewertungen
- PaediatricsDokument181 SeitenPaediatricsChukwuogo AkanegbuNoch keine Bewertungen
- Basic Principles of Periodontal SurgeryDokument100 SeitenBasic Principles of Periodontal SurgerySandip Ladani100% (2)
- Topical Corticosteroids For Childhood Eczema:: Clearing Up The ConfusionDokument6 SeitenTopical Corticosteroids For Childhood Eczema:: Clearing Up The ConfusionRed DiggerNoch keine Bewertungen