Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Review Article: Uveitis in The Aging Eye: Incidence, Patterns, and Differential DiagnosisDokument8 SeitenReview Article: Uveitis in The Aging Eye: Incidence, Patterns, and Differential DiagnosisRegina SeptianiNoch keine Bewertungen
- Ni Hms 597871Dokument20 SeitenNi Hms 597871Regina SeptianiNoch keine Bewertungen
- Practice: Bilateral Peritonsillar Abscesses Complicating Acute TonsillitisDokument4 SeitenPractice: Bilateral Peritonsillar Abscesses Complicating Acute TonsillitisRegina SeptianiNoch keine Bewertungen
- C.5 Encopresis 0072012Dokument14 SeitenC.5 Encopresis 0072012Indah Afriani Nasution100% (1)
- Case Report: Plasenta PreviaDokument2 SeitenCase Report: Plasenta PreviaRegina SeptianiNoch keine Bewertungen
- Enzyme - 2: Aspect Molecular of EnzymeDokument14 SeitenEnzyme - 2: Aspect Molecular of EnzymeRegina SeptianiNoch keine Bewertungen
- Enzyme - 2: Aspect Molecular of EnzymeDokument14 SeitenEnzyme - 2: Aspect Molecular of EnzymeRegina SeptianiNoch keine Bewertungen
- Death After Head Injury: The 13 Year Outcome of A Case Control StudyDokument6 SeitenDeath After Head Injury: The 13 Year Outcome of A Case Control StudyRegina SeptianiNoch keine Bewertungen
- Jurnal Reading: Efek ACE Inhibitor (Zofenopril) Terhadap Mortalitas Dan Morbiditas Setelah Infark Miokard AnteriorDokument1 SeiteJurnal Reading: Efek ACE Inhibitor (Zofenopril) Terhadap Mortalitas Dan Morbiditas Setelah Infark Miokard AnteriorRegina SeptianiNoch keine Bewertungen
- Emergency THTDokument37 SeitenEmergency THTIndah D. RahmahNoch keine Bewertungen
- Magnesium Intake and Colorectal Tumor Risk: A Case-Control Study and Meta-AnalysisDokument10 SeitenMagnesium Intake and Colorectal Tumor Risk: A Case-Control Study and Meta-AnalysisRegina SeptianiNoch keine Bewertungen
- Jurnal Retinopati DiabetikDokument11 SeitenJurnal Retinopati DiabetikAzwaydaRayhanaSariNoch keine Bewertungen
- Laparoscopic-Assisted Versus Open Surgery For Colorectal Cancer: Short-And Long-Term Outcomes ComparisonDokument7 SeitenLaparoscopic-Assisted Versus Open Surgery For Colorectal Cancer: Short-And Long-Term Outcomes ComparisonRegina SeptianiNoch keine Bewertungen
- Colorectal 4Dokument6 SeitenColorectal 4Regina SeptianiNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- LTE Principle and LTE PlanningDokument70 SeitenLTE Principle and LTE PlanningShain SalimNoch keine Bewertungen
- Bomba Watson Marlow PDFDokument13 SeitenBomba Watson Marlow PDFRonald SalasNoch keine Bewertungen
- IOCL JEA Recruitment 2021: Notification For 500+ Post, Apply Online From 21 SeptemberDokument10 SeitenIOCL JEA Recruitment 2021: Notification For 500+ Post, Apply Online From 21 SeptemberRajesh K KumarNoch keine Bewertungen
- Memperkuat Nasionalisme Indonesia Di Era Globalisasi ) Oleh Dwi Ari Listyani. )Dokument20 SeitenMemperkuat Nasionalisme Indonesia Di Era Globalisasi ) Oleh Dwi Ari Listyani. )PinaSeeYouNoch keine Bewertungen
- Tectos Falsos Stretch Caracteristicas TecnicasDokument37 SeitenTectos Falsos Stretch Caracteristicas TecnicasVadymNoch keine Bewertungen
- Santrock Section 1 Chapter 1Dokument19 SeitenSantrock Section 1 Chapter 1Assumpta Minette Burgos75% (8)
- Part DDokument6 SeitenPart DKaranja KinyanjuiNoch keine Bewertungen
- Principle of ManagementsDokument77 SeitenPrinciple of ManagementsJayson LucenaNoch keine Bewertungen
- All About Me - RubricDokument3 SeitenAll About Me - Rubricapi-314921155Noch keine Bewertungen
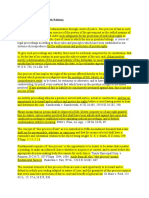
- Due Process of LawDokument2 SeitenDue Process of Lawjoe100% (4)
- 2016 Biology CheckpointDokument14 Seiten2016 Biology CheckpointNicholas Leong100% (1)
- FOR of Tution Fee: Application ReimbursementDokument1 SeiteFOR of Tution Fee: Application ReimbursementBhavithavNoch keine Bewertungen
- Probet DocxuDokument12 SeitenProbet DocxuAbuuAwadhNoch keine Bewertungen
- Areopagitica - John MiltonDokument1 SeiteAreopagitica - John MiltonwehanNoch keine Bewertungen
- Holidays Homework 12Dokument26 SeitenHolidays Homework 12richa agarwalNoch keine Bewertungen
- Thesis For Driving AgeDokument6 SeitenThesis For Driving Agestefanieyangmanchester100% (2)
- Latihan Soal CausativeDokument1 SeiteLatihan Soal Causativeanakosagista anakosagistaNoch keine Bewertungen
- Aficionado PERDokument19 SeitenAficionado PERMaecaella LlorenteNoch keine Bewertungen
- Further Investigations of Glucose-6-Phosphate Dehy PDFDokument7 SeitenFurther Investigations of Glucose-6-Phosphate Dehy PDFrabin1994Noch keine Bewertungen
- Death and Dying: Presented by Dr. Judith SugayDokument21 SeitenDeath and Dying: Presented by Dr. Judith SugayMichelle HutamaresNoch keine Bewertungen
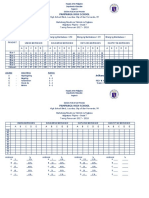
- Silent Reading With Graph1Dokument2 SeitenSilent Reading With Graph1JonaldSamueldaJoseNoch keine Bewertungen
- 2202 Infantilization Essay - Quinn WilsonDokument11 Seiten2202 Infantilization Essay - Quinn Wilsonapi-283151250Noch keine Bewertungen
- Preview ISO+15613-2004Dokument6 SeitenPreview ISO+15613-2004Brijith0% (1)
- EY Global Hospitality Insights 2016Dokument24 SeitenEY Global Hospitality Insights 2016Anonymous BkmsKXzwyKNoch keine Bewertungen
- Eapp Las Q3 Week 1Dokument8 SeitenEapp Las Q3 Week 1Maricel VallejosNoch keine Bewertungen
- HG G2 Q1 W57 Module 3 RTPDokument11 SeitenHG G2 Q1 W57 Module 3 RTPJennilyn Amable Democrito100% (1)
- CWWDokument2 SeitenCWWmary joy martinNoch keine Bewertungen
- Nursing Philosophy Apa PaperDokument7 SeitenNursing Philosophy Apa Paperapi-449016836Noch keine Bewertungen
- Direct Method (Education) : Navigation SearchDokument5 SeitenDirect Method (Education) : Navigation Searcheisha_91Noch keine Bewertungen
- Syntax 1Dokument35 SeitenSyntax 1galcarolina722202100% (1)