Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Psychiatry PhyseoDokument60 SeitenPsychiatry PhyseoGautam ManoharNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Thomas Pynchon-The Crying Lot of 49Dokument56 SeitenThomas Pynchon-The Crying Lot of 49RobertoBanda100% (3)
- Psychiatric History and Mental Status Examination GuideDokument7 SeitenPsychiatric History and Mental Status Examination GuideGabriel Gerardo N. Cortez100% (1)
- Introduction To MicrobiologyDokument27 SeitenIntroduction To MicrobiologyNicoel67% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Thyroid Disorder in Medical Astrology - Jyotish Surfer PDFDokument40 SeitenThyroid Disorder in Medical Astrology - Jyotish Surfer PDFAria AriaNoch keine Bewertungen
- Drug AbuseDokument5 SeitenDrug AbuseSajeel ZamanNoch keine Bewertungen
- GIT CASE TakingDokument19 SeitenGIT CASE TakingchanNoch keine Bewertungen
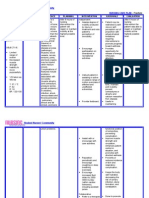
- Nursing Care Plan - FractureDokument2 SeitenNursing Care Plan - Fracturederic95% (19)
- Amikacin antibiotic for urinary tract infectionsDokument17 SeitenAmikacin antibiotic for urinary tract infectionsMc Crister SilangNoch keine Bewertungen
- SCE Nephrology Sample Questions 51-70 PDFDokument18 SeitenSCE Nephrology Sample Questions 51-70 PDFayo odeyemiNoch keine Bewertungen
- Linagliptin - DRUG STUDYDokument1 SeiteLinagliptin - DRUG STUDYAcads useNoch keine Bewertungen
- Pathology and GeneticsDokument11 SeitenPathology and Geneticssingireddi1revathi33% (3)
- Helping Mothers BreastfeedDokument23 SeitenHelping Mothers Breastfeed.Noch keine Bewertungen
- Degenerative Diseases of SpineDokument115 SeitenDegenerative Diseases of SpineCodillia CheongNoch keine Bewertungen
- Cholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarDokument25 SeitenCholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarMc Crister Silang100% (1)
- Schistosomiasis (From Anatomy To Pathophysiology)Dokument10 SeitenSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Dementia (Course Requirement Elective)Dokument21 SeitenDementia (Course Requirement Elective)Mc Crister SilangNoch keine Bewertungen
- Transition To IndependenceDokument14 SeitenTransition To IndependenceMc Crister SilangNoch keine Bewertungen
- Normal ValuesDokument6 SeitenNormal ValuesMc Crister SilangNoch keine Bewertungen
- In The Totality Paradigm Rosemarie ParseDokument2 SeitenIn The Totality Paradigm Rosemarie ParseMc Crister Silang43% (7)
- Gallbladder CancerDokument4 SeitenGallbladder CancerMc Crister SilangNoch keine Bewertungen
- Preoperative Skin PreparationDokument5 SeitenPreoperative Skin PreparationMc Crister SilangNoch keine Bewertungen
- Artificial Kidney CareDokument23 SeitenArtificial Kidney CareMc Crister SilangNoch keine Bewertungen
- Drug Information SummaryDokument10 SeitenDrug Information SummaryMc Crister SilangNoch keine Bewertungen
- Gallbladder Cancer MedscapeDokument7 SeitenGallbladder Cancer MedscapeMc Crister SilangNoch keine Bewertungen
- Nursing Care Plan To The Client With Fractures of The Extremities and Extremities SurgeryDokument2 SeitenNursing Care Plan To The Client With Fractures of The Extremities and Extremities SurgeryMaria MedinaNoch keine Bewertungen
- Drug StudyDokument36 SeitenDrug StudyMc Crister SilangNoch keine Bewertungen
- Same Sex MarriageDokument1 SeiteSame Sex MarriageMc Crister SilangNoch keine Bewertungen
- of UrinaryDokument42 Seitenof UrinaryMc Crister SilangNoch keine Bewertungen
- LaringitisDokument14 SeitenLaringitisrico doloksaribuNoch keine Bewertungen
- CLINDA DRUG STUDYDokument6 SeitenCLINDA DRUG STUDYMa. Rita Concepcion TungulNoch keine Bewertungen
- HypoglycemiaDokument12 SeitenHypoglycemiaNTA UGC-NETNoch keine Bewertungen
- Physio Ex 8.0 Exercise 7 WorksheetDokument11 SeitenPhysio Ex 8.0 Exercise 7 WorksheetCDN50% (2)
- Intermittent FastingDokument13 SeitenIntermittent FastingGina DeStefano RolfsmeierNoch keine Bewertungen
- Team C Final Written OutputDokument22 SeitenTeam C Final Written OutputCarina SuarezNoch keine Bewertungen
- Health Questionnaire TemplateDokument2 SeitenHealth Questionnaire TemplateBaxwal AxmedNoch keine Bewertungen
- Paragraph Writing: G.P.Ragini Senior Assistant Professor School of Humanities and Sciences SASTRA UniversityDokument6 SeitenParagraph Writing: G.P.Ragini Senior Assistant Professor School of Humanities and Sciences SASTRA UniversityGeomanjeriNoch keine Bewertungen
- The Muscular System: Medical AssistingDokument60 SeitenThe Muscular System: Medical AssistingMeme YuNoch keine Bewertungen
- Heat Illness Quiz 070716Dokument2 SeitenHeat Illness Quiz 070716Trent HairNoch keine Bewertungen
- Malaria Case AnalysisDokument1 SeiteMalaria Case AnalysisANGELA MARIE VILLENANoch keine Bewertungen
- Ulcerative Colitis Causes, Symptoms, and Risk Factors ExplainedDokument1 SeiteUlcerative Colitis Causes, Symptoms, and Risk Factors ExplainedDolly MadisonNoch keine Bewertungen
- The Starch Solution: A Widely Tested Vegan Diet for Reversing DiseaseDokument2 SeitenThe Starch Solution: A Widely Tested Vegan Diet for Reversing DiseaseSalman khanNoch keine Bewertungen
- PreviewpdfDokument23 SeitenPreviewpdfKhaalid AbdirahmanNoch keine Bewertungen
- HEMOFLAGELLATESDokument5 SeitenHEMOFLAGELLATESmkct111Noch keine Bewertungen
- Crohn's DiseaseDokument1 SeiteCrohn's DiseaseibrahimNoch keine Bewertungen
- The Importance of Food Safety, Hygiene and Sanitation in Making LambanogDokument13 SeitenThe Importance of Food Safety, Hygiene and Sanitation in Making LambanogJayson Fabrigas VillafrancaNoch keine Bewertungen
- ProvimiDokument13 SeitenProvimialbert lukaNoch keine Bewertungen