Das könnte Ihnen auch gefallen
- TermsDokument6 SeitenTermsshaikh javedNoch keine Bewertungen
- My PresentationDokument8 SeitenMy Presentationshaikh javedNoch keine Bewertungen
- Chap # 1 - Introduction To Entrepreneurship (Edited)Dokument41 SeitenChap # 1 - Introduction To Entrepreneurship (Edited)shaikh javedNoch keine Bewertungen
- Apple's Five Forces Analysis Reveals Competitive Rivalry and Buyer Power as Key External FactorsDokument3 SeitenApple's Five Forces Analysis Reveals Competitive Rivalry and Buyer Power as Key External Factorsshaikh javedNoch keine Bewertungen
- Intro To Research PDFDokument19 SeitenIntro To Research PDFshaikh javedNoch keine Bewertungen
- Chap # 1 - Introduction To Entrepreneurship (Edited)Dokument41 SeitenChap # 1 - Introduction To Entrepreneurship (Edited)shaikh javedNoch keine Bewertungen
- My PresentationDokument8 SeitenMy Presentationshaikh javedNoch keine Bewertungen
- Basic Research: Presented by Manu AliasDokument11 SeitenBasic Research: Presented by Manu Aliasshaikh javedNoch keine Bewertungen
- Research Methods Chapter #09Dokument39 SeitenResearch Methods Chapter #09shaikh javedNoch keine Bewertungen
- Shaheed Benazir Bhutto University, Shaheed BenazirabadDokument1 SeiteShaheed Benazir Bhutto University, Shaheed Benazirabadshaikh javedNoch keine Bewertungen
- Personality Tests AnnouncementsDokument36 SeitenPersonality Tests Announcementsshaikh javedNoch keine Bewertungen
- Difference Between International, Multinational and Global CompaniesDokument1 SeiteDifference Between International, Multinational and Global Companiesshaikh javedNoch keine Bewertungen
- Basic Research: Presented by Manu AliasDokument11 SeitenBasic Research: Presented by Manu Aliasshaikh javedNoch keine Bewertungen
- Strategic Management Case SkodaDokument4 SeitenStrategic Management Case SkodaymmahmudNoch keine Bewertungen
- Shaheed Benazir Bhutto University, Shaheed BenazirabadDokument1 SeiteShaheed Benazir Bhutto University, Shaheed Benazirabadshaikh javedNoch keine Bewertungen
- Customer Relationship Management: Acknowledgements To Euan Wilson (Staffordshire University)Dokument18 SeitenCustomer Relationship Management: Acknowledgements To Euan Wilson (Staffordshire University)Neha BhograNoch keine Bewertungen
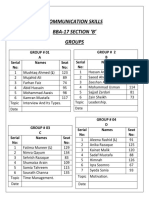
- Communication Skills Bba-17 Section B' GroupsDokument2 SeitenCommunication Skills Bba-17 Section B' Groupsshaikh javedNoch keine Bewertungen
- Modern Management Theories and PracticesDokument25 SeitenModern Management Theories and PracticesSyed Waqar Akbar Tirmizi100% (4)
- Exam QuestionDokument10 SeitenExam Questionshaikh javedNoch keine Bewertungen
- Abstract of ExtremismDokument3 SeitenAbstract of Extremismshaikh javedNoch keine Bewertungen
- A Glossary of Terms Used in Brand ManagementDokument3 SeitenA Glossary of Terms Used in Brand ManagementWasipfcNoch keine Bewertungen
- Subject: Application For The Post of Management TraineeDokument1 SeiteSubject: Application For The Post of Management Traineeshaikh javedNoch keine Bewertungen
- OGDCL ProductionAug14Dokument1 SeiteOGDCL ProductionAug14Muhammad AliNoch keine Bewertungen
- CHPT 7 Products and ServicesDokument58 SeitenCHPT 7 Products and Servicesshaikh javedNoch keine Bewertungen
- Packaging ElementsDokument1 SeitePackaging Elementsshaikh javedNoch keine Bewertungen
- Javed Ahmed Shaikh: Chapter 1-Slide 1Dokument19 SeitenJaved Ahmed Shaikh: Chapter 1-Slide 1shaikh javedNoch keine Bewertungen
- AdvertismentDokument4 SeitenAdvertismentshaikh javedNoch keine Bewertungen
- Air Asia FinalDokument21 SeitenAir Asia FinalIshmail People's33% (3)
- None of AboveDokument4 SeitenNone of Aboveshaikh javedNoch keine Bewertungen
- Air Asia's Low-Cost Leadership StrategyDokument8 SeitenAir Asia's Low-Cost Leadership StrategyLaila Al-Alawi80% (5)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Insulin Lecture For RHUDokument13 SeitenInsulin Lecture For RHUCJ BunoanNoch keine Bewertungen
- Bailey ResumeeDokument3 SeitenBailey Resumeeapi-314996796Noch keine Bewertungen
- Murder Mystery LabDokument19 SeitenMurder Mystery Labapi-451038689Noch keine Bewertungen
- 2012 Near DrowningDokument35 Seiten2012 Near Drowningkamel6100% (1)
- Discharge Instruction: Learning ObjectiveDokument7 SeitenDischarge Instruction: Learning ObjectiveKampus 2 RS. CiremaiNoch keine Bewertungen
- Venous Thromboembolism in Pregnancy: EpidemiologyDokument8 SeitenVenous Thromboembolism in Pregnancy: EpidemiologyKhalil KhusairiNoch keine Bewertungen
- Rhopalurus Junceus: and The Treatment of CancerDokument17 SeitenRhopalurus Junceus: and The Treatment of CancerAmalia Tri UtamiNoch keine Bewertungen
- ERCP ExplainedDokument4 SeitenERCP ExplainedMichelle TamorNoch keine Bewertungen
- CLASSIFYING GASTRITISDokument40 SeitenCLASSIFYING GASTRITISmadalinamihaiNoch keine Bewertungen
- Rights and Responsibilities of Health Care ProvidersDokument2 SeitenRights and Responsibilities of Health Care ProvidersAlondra Sagario0% (1)
- Open Structure Rhinoplasty For Management of The Non-Caucasian NoseDokument9 SeitenOpen Structure Rhinoplasty For Management of The Non-Caucasian NoseJose ManuelNoch keine Bewertungen
- Course Syllabus (Sample)Dokument11 SeitenCourse Syllabus (Sample)Gelaie Salangsang100% (3)
- ICU LogbookDokument37 SeitenICU Logbookrinus5100% (1)
- IDS Inmediate Dentin Sealing For Tooth Preparations... Magne 2014Dokument2 SeitenIDS Inmediate Dentin Sealing For Tooth Preparations... Magne 2014Angie HernándezNoch keine Bewertungen
- Medical Prioritization ProcessDokument20 SeitenMedical Prioritization ProcessIGDNoch keine Bewertungen
- Reading Test 1 - Part A': Page - 1Dokument14 SeitenReading Test 1 - Part A': Page - 1Ryu Tse100% (2)
- International Guidelines For Groin Hernia ManagementDokument165 SeitenInternational Guidelines For Groin Hernia ManagementDina100% (1)
- Andre Hannah NursingresumeDokument1 SeiteAndre Hannah Nursingresumeapi-450112281Noch keine Bewertungen
- Joyce Travelbee: Human-to-Human RelationshipDokument20 SeitenJoyce Travelbee: Human-to-Human RelationshipJamesBuensalidoDellavaNoch keine Bewertungen
- Time, Final Rinse Protocol and EndodonticsDokument1 SeiteTime, Final Rinse Protocol and EndodonticsvaamdevaaNoch keine Bewertungen
- Closed Tibia and Fibula Fractures in 44-Year-Old Male PatientDokument25 SeitenClosed Tibia and Fibula Fractures in 44-Year-Old Male Patientleonard0% (1)
- Toxi TestDokument4 SeitenToxi TestFrank NobodNoch keine Bewertungen
- Diagnostic Peritoneal Lavage (DPL)Dokument10 SeitenDiagnostic Peritoneal Lavage (DPL)hatem alsrour100% (2)
- Cardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionDokument8 SeitenCardiopulmonary Resuscitation: Unusual Techniques For Unusual Situations ConclusionIlham AkbarNoch keine Bewertungen
- 'NEXtCARE UAE - ASOAP FormDokument1 Seite'NEXtCARE UAE - ASOAP FormMohyee Eldin RagebNoch keine Bewertungen
- Ashley Jones RN ResumeDokument1 SeiteAshley Jones RN Resumeapi-299649525100% (1)
- NorepinephrineDokument4 SeitenNorepinephrineLoids IgnacioNoch keine Bewertungen
- Anamnesis & PemfisDokument81 SeitenAnamnesis & PemfisFikriYTNoch keine Bewertungen
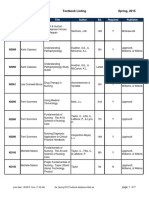
- BFLSON Course Textbook ListingDokument7 SeitenBFLSON Course Textbook ListingWina ViqaNoch keine Bewertungen
- Pediatric Fluid and Electrolyte AlterationsDokument51 SeitenPediatric Fluid and Electrolyte AlterationsMatthew Ryan100% (1)