Das könnte Ihnen auch gefallen
- Porters Five Force ModelDokument3 SeitenPorters Five Force Modelshaikh javedNoch keine Bewertungen
- Shaheed Benazir Bhutto University, Shaheed BenazirabadDokument1 SeiteShaheed Benazir Bhutto University, Shaheed Benazirabadshaikh javedNoch keine Bewertungen
- Chap # 1 - Introduction To Entrepreneurship (Edited)Dokument41 SeitenChap # 1 - Introduction To Entrepreneurship (Edited)shaikh javedNoch keine Bewertungen
- Chap # 1 - Introduction To Entrepreneurship (Edited)Dokument41 SeitenChap # 1 - Introduction To Entrepreneurship (Edited)shaikh javedNoch keine Bewertungen
- Intro To Research PDFDokument19 SeitenIntro To Research PDFshaikh javedNoch keine Bewertungen
- AnnouncementsDokument36 SeitenAnnouncementsshaikh javedNoch keine Bewertungen
- Shaheed Benazir Bhutto University, Shaheed BenazirabadDokument1 SeiteShaheed Benazir Bhutto University, Shaheed Benazirabadshaikh javedNoch keine Bewertungen
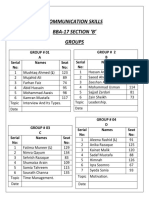
- Communication Skills Bba-17 Section B' GroupsDokument2 SeitenCommunication Skills Bba-17 Section B' Groupsshaikh javedNoch keine Bewertungen
- Basic Research: Presented by Manu AliasDokument11 SeitenBasic Research: Presented by Manu Aliasshaikh javedNoch keine Bewertungen
- Difference Between International, Multinational and Global CompaniesDokument1 SeiteDifference Between International, Multinational and Global Companiesshaikh javedNoch keine Bewertungen
- None of AboveDokument4 SeitenNone of Aboveshaikh javedNoch keine Bewertungen
- Rewards and Employee Motivation-Nirma UniversityDokument17 SeitenRewards and Employee Motivation-Nirma Universityshaikh javed100% (1)
- Javed Ahmed Shaikh: Chapter 1-Slide 1Dokument19 SeitenJaved Ahmed Shaikh: Chapter 1-Slide 1shaikh javedNoch keine Bewertungen
- Subject: Application For The Post of Management TraineeDokument1 SeiteSubject: Application For The Post of Management Traineeshaikh javedNoch keine Bewertungen
- Od HeadsDokument1 SeiteOd Headsshaikh javedNoch keine Bewertungen
- Research Methods Chapter #09Dokument39 SeitenResearch Methods Chapter #09shaikh javedNoch keine Bewertungen
- Performance AppraisalDokument7 SeitenPerformance Appraisalshaikh javedNoch keine Bewertungen
- BF CS Credit Card Cross Sell WEB 0Dokument2 SeitenBF CS Credit Card Cross Sell WEB 0shaikh javedNoch keine Bewertungen
- SMP Report On Tapal TeaDokument48 SeitenSMP Report On Tapal Teashaikh javedNoch keine Bewertungen
- Ishrat HussainDokument14 SeitenIshrat Hussainshaikh javedNoch keine Bewertungen
- Distribution Channels, Roles of Sales Teams/Branch Bankers & Retention of TeamsDokument14 SeitenDistribution Channels, Roles of Sales Teams/Branch Bankers & Retention of Teamsshaikh javedNoch keine Bewertungen
- The Crisis of Internally Displaced Persons (Idps) in The Federally Administered Tribal Areas of Pakistan and Their Impact On Pashtun WomenDokument26 SeitenThe Crisis of Internally Displaced Persons (Idps) in The Federally Administered Tribal Areas of Pakistan and Their Impact On Pashtun Womenshaikh javedNoch keine Bewertungen
- Ram Charan FortuneDokument10 SeitenRam Charan Fortuneshaikh javedNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Tricks To Remember Important Days-All-MonthsDokument2 SeitenTricks To Remember Important Days-All-MonthsSenthikumar MuraliNoch keine Bewertungen
- Personal StatementDokument1 SeitePersonal StatementTaiwo Oyeniyi100% (2)
- Deep BretahingDokument4 SeitenDeep Bretahingagustina ika100% (1)
- Endocrine: QuestionsDokument14 SeitenEndocrine: QuestionsMuhammad Abubakar100% (1)
- Ncbi Selulitis BulosaDokument3 SeitenNcbi Selulitis BulosaHarefa TirtaNoch keine Bewertungen
- Metabolic Acidosis FinalDokument29 SeitenMetabolic Acidosis FinalTera SurbaktiNoch keine Bewertungen
- Amla As A Health FoodDokument14 SeitenAmla As A Health FoodKUNAL MITTALNoch keine Bewertungen
- Meal Plan Medyo FinalDokument14 SeitenMeal Plan Medyo FinalJasha MaeNoch keine Bewertungen
- Unidirctional Anti Covid-19 Gate Using Motion SensorDokument45 SeitenUnidirctional Anti Covid-19 Gate Using Motion SensorMuhammad SalmanNoch keine Bewertungen
- TRS601 Vocabulary ListDokument5 SeitenTRS601 Vocabulary ListNgo Van Hung (K17 HCM)Noch keine Bewertungen
- Pharmacology of Drugs Acting On Renal SystemDokument20 SeitenPharmacology of Drugs Acting On Renal SystemBestha Chakri100% (2)
- Reactive ArthritisDokument8 SeitenReactive ArthritisamereNoch keine Bewertungen
- Environmental Hazards Assignment Winter Quarter 2015-16Dokument32 SeitenEnvironmental Hazards Assignment Winter Quarter 2015-16Muhammad AbbasNoch keine Bewertungen
- Script For OrientationDokument2 SeitenScript For OrientationAngela CudiaNoch keine Bewertungen
- Classification of Psychiatric DisordersDokument64 SeitenClassification of Psychiatric Disordersdrkadiyala2100% (1)
- Saudi License Exam (SLE) For General Dentistry - Sep 6, 2011Dokument10 SeitenSaudi License Exam (SLE) For General Dentistry - Sep 6, 2011asifhameed90% (10)
- Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualDokument12 SeitenChildhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualJenniferAguilarrfiax100% (10)
- Fix Daftar PustakaDokument6 SeitenFix Daftar Pustakaeka saptaning windu fitriNoch keine Bewertungen
- Pulp Therapy in ChildrenDokument4 SeitenPulp Therapy in ChildrenshahinshamshiriNoch keine Bewertungen
- The Role of Advertising in High-Tech Medical Procedures: Evidence From Robotic SurgeriesDokument79 SeitenThe Role of Advertising in High-Tech Medical Procedures: Evidence From Robotic SurgeriesEve AthanasekouNoch keine Bewertungen
- Galvano-Spa-Bath and HealthDokument2 SeitenGalvano-Spa-Bath and HealthDeu na telha com Janaína BensdorpNoch keine Bewertungen
- Plectranthus Amboinicus: A Review On Its Pharmacological And, Pharmacognostical StudiesDokument9 SeitenPlectranthus Amboinicus: A Review On Its Pharmacological And, Pharmacognostical StudiesMuhammad UmerNoch keine Bewertungen
- Entrez Digital Tools and UtilitiesDokument80 SeitenEntrez Digital Tools and UtilitiesGeorge Sebastian AntonyNoch keine Bewertungen
- Plasmodium Infection (Malaria) : Medical ParasitologyDokument7 SeitenPlasmodium Infection (Malaria) : Medical ParasitologyBalisi Manuel FranciscoNoch keine Bewertungen
- Paracetamol Induced Steven-Johnson Syndrome: A Rare Case ReportDokument4 SeitenParacetamol Induced Steven-Johnson Syndrome: A Rare Case ReportDorainne JohnsonNoch keine Bewertungen
- Kinesiology Tape Guide - Physix Gear Sport PDFDokument85 SeitenKinesiology Tape Guide - Physix Gear Sport PDFTomas Delfiner100% (1)
- Management of Cancer (Dr. Lim)Dokument6 SeitenManagement of Cancer (Dr. Lim)Miguel Cuevas DolotNoch keine Bewertungen
- Calamansi and Lemongrass As Alternative Mosquito Coil: Submitted By: Kristhel Nieves N. Zamora 10-AmethystDokument6 SeitenCalamansi and Lemongrass As Alternative Mosquito Coil: Submitted By: Kristhel Nieves N. Zamora 10-AmethystKristhel ZamoraNoch keine Bewertungen
- Transgenic AnimaliaDokument4 SeitenTransgenic AnimaliaGalino Julia Cristine A.Noch keine Bewertungen