Das könnte Ihnen auch gefallen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Managing Asthma in Anaesthesia: Key ConsiderationsDokument39 SeitenManaging Asthma in Anaesthesia: Key ConsiderationsParvathy R NairNoch keine Bewertungen
- A02 453Dokument22 SeitenA02 453jaimeNoch keine Bewertungen
- Drugs For AsthmaDokument7 SeitenDrugs For Asthmaapi-3736350Noch keine Bewertungen
- Bronchodilators and Other Respiratory AgentsDokument46 SeitenBronchodilators and Other Respiratory AgentsElthon John BueNoch keine Bewertungen
- Bronchodilator & Other Drugs Used in AsthmaDokument15 SeitenBronchodilator & Other Drugs Used in AsthmaGenta JagadNoch keine Bewertungen
- Drugs For Chronic ObstructiveDokument57 SeitenDrugs For Chronic ObstructivedhaineyNoch keine Bewertungen
- Asthma Pathophysiology: Ixsy Ramirez, MD, MPH Pediatric Pulmonology University of Michigan, C.S. Mott Children's HospitalDokument21 SeitenAsthma Pathophysiology: Ixsy Ramirez, MD, MPH Pediatric Pulmonology University of Michigan, C.S. Mott Children's HospitalAru VermaNoch keine Bewertungen
- Child asthma discharge care guideDokument15 SeitenChild asthma discharge care guideJu Lie AnnNoch keine Bewertungen
- Paediatric AsthmaDokument246 SeitenPaediatric AsthmaOxana TurcuNoch keine Bewertungen
- AsthmaDokument46 SeitenAsthmaHafiz Muhammad AeymonNoch keine Bewertungen
- Asthma Review PDFDokument12 SeitenAsthma Review PDFdanielc503Noch keine Bewertungen
- EAC BASIC Respiratory Pharmacology DrugsDokument130 SeitenEAC BASIC Respiratory Pharmacology DrugsMARK RYAN HERNANDEZNoch keine Bewertungen
- Bronchoconstrictor Additives in Bronchodilator SolutionsDokument8 SeitenBronchoconstrictor Additives in Bronchodilator SolutionsHisyamAl-MuhammadiNoch keine Bewertungen
- Asthma Ineffective Airway ClearanceDokument2 SeitenAsthma Ineffective Airway ClearanceEdmr SlzarNoch keine Bewertungen
- Asthma and COPD NCLEXDokument17 SeitenAsthma and COPD NCLEXPotchiee PfizerNoch keine Bewertungen
- Bronchial AsthmaDokument11 SeitenBronchial AsthmaFaria Islam JuhiNoch keine Bewertungen
- Asthma PathophysiologyDokument4 SeitenAsthma Pathophysiologysmitha lakkavallyNoch keine Bewertungen
- Diagnosis and Management of Asthma in AdultsDokument12 SeitenDiagnosis and Management of Asthma in AdultsRoberto López Mata67% (6)
- ASTHMADokument17 SeitenASTHMAvinda astri permatasariNoch keine Bewertungen
- 26.pulmonary PharmacologyDokument14 Seiten26.pulmonary PharmacologyAnggreany AshariNoch keine Bewertungen
- Chapter 55 - Drugs Acting On The Lower Respiratory TractDokument13 SeitenChapter 55 - Drugs Acting On The Lower Respiratory TractJonathonNoch keine Bewertungen
- Ipratropium BromidaDokument2 SeitenIpratropium BromidaHarum Binar MetrikasantiNoch keine Bewertungen
- Wa0005.Dokument4 SeitenWa0005.science worldNoch keine Bewertungen
- Anti Asthmatic DrugsDokument8 SeitenAnti Asthmatic DrugsNavjot BrarNoch keine Bewertungen
- Drugs for Cough, Bronchial Asthma and InflammationDokument47 SeitenDrugs for Cough, Bronchial Asthma and InflammationNavlika DuttaNoch keine Bewertungen
- Nurs 5002 - Case Study 4Dokument17 SeitenNurs 5002 - Case Study 4api-308904543100% (2)
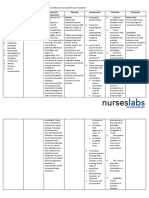
- Bronchial Asthma Nursing Care PlansDokument2 SeitenBronchial Asthma Nursing Care PlansdeincediannaNoch keine Bewertungen
- Asthma: Signs and SymptomsDokument57 SeitenAsthma: Signs and SymptomsAjp Ryuzaki CaesarNoch keine Bewertungen
- Asthma + COPDDokument60 SeitenAsthma + COPDNur HasanahNoch keine Bewertungen
- PBL Case 1Dokument11 SeitenPBL Case 1Irina Luciana DumitriuNoch keine Bewertungen