Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- VSIM Clinical Worksheet 07.16.2020Dokument6 SeitenVSIM Clinical Worksheet 07.16.2020Jackie GriffisNoch keine Bewertungen
- Whitepaper Top 10 Big Data Trends 2017Dokument13 SeitenWhitepaper Top 10 Big Data Trends 2017Andréa FagundesNoch keine Bewertungen
- A Collection of Studies On BonDokument103 SeitenA Collection of Studies On BonKabafi0% (1)
- Looking Toward Cyberspace: Beyond Grounded SociologyDokument7 SeitenLooking Toward Cyberspace: Beyond Grounded SociologyMaria Sri PangestutiNoch keine Bewertungen
- Looking Toward Cyberspace: Beyond Grounded SociologyDokument7 SeitenLooking Toward Cyberspace: Beyond Grounded SociologyMaria Sri PangestutiNoch keine Bewertungen
- (John Protevi) Political Physics Deleuze, DerridaDokument256 Seiten(John Protevi) Political Physics Deleuze, DerridajpirattaaNoch keine Bewertungen
- Kalachakra Initiation - Madison 1981 PDFDokument88 SeitenKalachakra Initiation - Madison 1981 PDFMaria Sri Pangestuti100% (3)
- 10 PDFDokument5 Seiten10 PDFMaria Sri PangestutiNoch keine Bewertungen
- Bouter De. K PDFDokument98 SeitenBouter De. K PDFMaria Sri PangestutiNoch keine Bewertungen
- The Body As A Text and The Text As The Body: A View From TheDokument24 SeitenThe Body As A Text and The Text As The Body: A View From ThealbertmelondiNoch keine Bewertungen
- 0001Dokument24 Seiten0001Roman Stanoev100% (3)
- Bouter De. K PDFDokument98 SeitenBouter De. K PDFMaria Sri PangestutiNoch keine Bewertungen
- Old Javanese Studies - Helen CreeseDokument32 SeitenOld Javanese Studies - Helen CreeseMaria Sri Pangestuti100% (1)
- Six CompetenciesDokument32 SeitenSix CompetenciesMaria Sri PangestutiNoch keine Bewertungen
- The Moon and Sixpence - Book - EngDokument324 SeitenThe Moon and Sixpence - Book - EngMaria Sri PangestutiNoch keine Bewertungen
- (John Protevi) Political Physics Deleuze, DerridaDokument256 Seiten(John Protevi) Political Physics Deleuze, DerridajpirattaaNoch keine Bewertungen
- Dalai Lama Kalachakra Teachings Day 1Dokument21 SeitenDalai Lama Kalachakra Teachings Day 1JohnIGodis0100% (1)
- Translation Is Not EnoughDokument46 SeitenTranslation Is Not EnoughMaria Sri PangestutiNoch keine Bewertungen
- American Buddhism As A Way of LifeDokument235 SeitenAmerican Buddhism As A Way of LifeFussa Dhaza100% (2)
- Broughton Jeffrey L. The Bodhidharma Anthology The Earliest Records of ZenBuddhismDokument91 SeitenBroughton Jeffrey L. The Bodhidharma Anthology The Earliest Records of ZenBuddhismphoenix1220100% (1)
- 2013 Managing Engagement During Times of Change White PaperDokument11 Seiten2013 Managing Engagement During Times of Change White PaperMaria Sri PangestutiNoch keine Bewertungen
- Buddhism in China by Whalen LAIDokument13 SeitenBuddhism in China by Whalen LAIMaria Sri Pangestuti100% (1)
- Broughton Jeffrey L. The Bodhidharma Anthology The Earliest Records of ZenBuddhismDokument91 SeitenBroughton Jeffrey L. The Bodhidharma Anthology The Earliest Records of ZenBuddhismphoenix1220100% (1)
- Machiavelli - Discourses On LivymansfieldDokument419 SeitenMachiavelli - Discourses On LivymansfieldMaria Sri Pangestuti100% (1)
- In The Search of Middle WayDokument70 SeitenIn The Search of Middle WayMaria Sri PangestutiNoch keine Bewertungen
- Deductionandreality - Patrick D BangertDokument279 SeitenDeductionandreality - Patrick D BangertMaria Sri PangestutiNoch keine Bewertungen
- Masaaki Hattori Dignaga, On Perception, Being The Pratyaksapariccheda of Dignagas Pramanasamuccaya From The Sanskrit Fragments and The Tibetan Versions PDFDokument279 SeitenMasaaki Hattori Dignaga, On Perception, Being The Pratyaksapariccheda of Dignagas Pramanasamuccaya From The Sanskrit Fragments and The Tibetan Versions PDFLucas Hernandes100% (1)
- Whither Psychoanalysis in Computer CultureDokument15 SeitenWhither Psychoanalysis in Computer CultureMaria Sri PangestutiNoch keine Bewertungen
- Hayes1994 - Nagarjuna Appeal PDFDokument80 SeitenHayes1994 - Nagarjuna Appeal PDFMaria Sri PangestutiNoch keine Bewertungen
- RAn Anarchist Introduction To Critical Race Theoryevolutionary Anti Authoritarians of Color An Anarchist Introduction To Critical Race TheoryDokument13 SeitenRAn Anarchist Introduction To Critical Race Theoryevolutionary Anti Authoritarians of Color An Anarchist Introduction To Critical Race TheoryMaria Sri PangestutiNoch keine Bewertungen
- Dignaga and Dharmakirti On ApohaDokument18 SeitenDignaga and Dharmakirti On ApohaMaria Sri PangestutiNoch keine Bewertungen
- A Case of Acute Ischemic Stroke With Left HemiparesisDokument18 SeitenA Case of Acute Ischemic Stroke With Left HemiparesisSafoora RafeeqNoch keine Bewertungen
- DokumenDokument4 SeitenDokumenFkep2015Noch keine Bewertungen
- Hydrotherapy Stroke ChinaDokument7 SeitenHydrotherapy Stroke China黃姵儒Noch keine Bewertungen
- Ischemic Stroke ManagementDokument8 SeitenIschemic Stroke ManagementBa LitNoch keine Bewertungen
- 2020 AFIB 2020 - For WebDokument166 Seiten2020 AFIB 2020 - For WebHussein TfNoch keine Bewertungen
- Ic VeastDokument11 SeitenIc VeastReza EbookNoch keine Bewertungen
- News004 Working Long Hours Kills Thousands Every YearDokument7 SeitenNews004 Working Long Hours Kills Thousands Every Yearsandra1975Noch keine Bewertungen
- Stroke Teaching Course: Brasov, Romania January 25-27, 2024Dokument4 SeitenStroke Teaching Course: Brasov, Romania January 25-27, 2024Catalina NastasaNoch keine Bewertungen
- Quackery, The 20 Million Dollar DuckDokument20 SeitenQuackery, The 20 Million Dollar DuckAustin Macauley Publishers Ltd.Noch keine Bewertungen
- Ayeni MotunrayoDokument5 SeitenAyeni Motunrayoayenimotunrayo40Noch keine Bewertungen
- 4 November 2004 DR - Supparearg DisayabutrDokument38 Seiten4 November 2004 DR - Supparearg DisayabutrDonnaya KrajangwittayaNoch keine Bewertungen
- Resuscitation: European Resuscitation Council Guidelines 2021: First AidDokument21 SeitenResuscitation: European Resuscitation Council Guidelines 2021: First AidLuis Fernando RodriguesNoch keine Bewertungen
- Case Study MeningitisDokument20 SeitenCase Study MeningitisMitch Love100% (5)
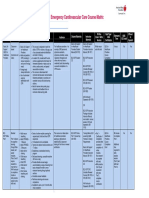
- Emergency Cardiovascular Care Course MatrixDokument15 SeitenEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaNoch keine Bewertungen
- AcstrokeDokument240 SeitenAcstrokeirinelirinelNoch keine Bewertungen
- Screen Capacity PaperDokument44 SeitenScreen Capacity PaperJuan FernándezNoch keine Bewertungen
- Geriatric Patient PDFDokument57 SeitenGeriatric Patient PDFHasan Al MasudNoch keine Bewertungen
- Nimesil PDFDokument5 SeitenNimesil PDFTemur LegendaryNoch keine Bewertungen
- Heart DiseasesDokument16 SeitenHeart DiseasesSanaNoch keine Bewertungen
- Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SDokument3 SeitenStroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery Sabu_abdisysyaakirNoch keine Bewertungen
- Stupor and Coma in AdultsDokument23 SeitenStupor and Coma in AdultsFdo RMNoch keine Bewertungen
- Neurology of Swallowing and DysphagiaDokument24 SeitenNeurology of Swallowing and DysphagiaMaríaFernandaCampanoGacitúaNoch keine Bewertungen
- Nursing Questions1Dokument17 SeitenNursing Questions1أبوأحمد الحكيمNoch keine Bewertungen
- Medical Tribune May 2013Dokument39 SeitenMedical Tribune May 2013Marissa WreksoatmodjoNoch keine Bewertungen
- Pe 1 Lesson 2 Non-Communicable DiseasesDokument79 SeitenPe 1 Lesson 2 Non-Communicable Diseasesdario serranoNoch keine Bewertungen
- CVA Case StudyDokument9 SeitenCVA Case Studypylzanne100% (1)
- Complete Occlusion of Extracranial Internal Carotid Artery: Clinical Features, Pathophysiology, Diagnosis and ManagementDokument5 SeitenComplete Occlusion of Extracranial Internal Carotid Artery: Clinical Features, Pathophysiology, Diagnosis and ManagementAndreea Raluca CimpoiNoch keine Bewertungen
- BB Marktstudie Medical Device Market in China 070215Dokument71 SeitenBB Marktstudie Medical Device Market in China 070215Deb BandyopadhyayNoch keine Bewertungen
- Tiki Taka Notes Final PDFDokument104 SeitenTiki Taka Notes Final PDFAditiSahak62Noch keine Bewertungen