Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- STUDENT LINKING WORDS AND PHRASESDokument6 SeitenSTUDENT LINKING WORDS AND PHRASESEdward YooNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
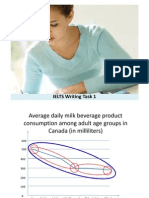
- IELTS Writing Answer SheetDokument4 SeitenIELTS Writing Answer SheetHighPoint IELTS Preparation Services, Inc.Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Essay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDokument5 SeitenEssay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDr-Usman Khan0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- TransitionsDokument3 SeitenTransitionsDr-Usman KhanNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- IELTS Speaking Part 1 VocabularyDokument24 SeitenIELTS Speaking Part 1 VocabularyDr-Usman Khan100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Nol 7zone Eng PDFDokument1 SeiteNol 7zone Eng PDFneedzinNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- YES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9Dokument6 SeitenYES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9YES IELTS100% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- IELTS True False Not GivenDokument5 SeitenIELTS True False Not GivenDr-Usman Khan100% (2)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Difference BTW False, No, NGDokument1 SeiteDifference BTW False, No, NGDr-Usman KhanNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Speaking Tips by RyanDokument2 SeitenSpeaking Tips by RyanDr-Usman Khan100% (3)
- Connectors For IELTSDokument24 SeitenConnectors For IELTSDr-Usman KhanNoch keine Bewertungen
- Difference BTW False, No, NGDokument1 SeiteDifference BTW False, No, NGDr-Usman KhanNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
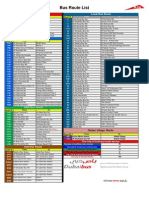
- Bus Route List EnglishDokument1 SeiteBus Route List EnglishDr-Usman KhanNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Bus Route List EnglishDokument1 SeiteBus Route List EnglishDr-Usman KhanNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Exam MaterialsDokument4 SeitenExam MaterialsDr-Usman KhanNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- PharmaciesDokument18 SeitenPharmaciesDr-Usman KhanNoch keine Bewertungen
- 32 Ielts Essay Samples Band 9Dokument34 Seiten32 Ielts Essay Samples Band 9mh73% (26)
- Delcaration Form by The Sponsoring FacilityDokument1 SeiteDelcaration Form by The Sponsoring FacilityDr-Usman Khan100% (1)
- 06 MarchDokument3 Seiten06 MarchDr-Usman Khan0% (1)
- 23 QsDokument8 Seiten23 QsDr-Usman Khan0% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 5 2 2014 - 2Dokument2 Seiten5 2 2014 - 2Dr-Usman Khan100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- 5 2 2014 - 2Dokument2 Seiten5 2 2014 - 2Dr-Usman Khan100% (1)
- 570 Academic Word List For IELTSDokument26 Seiten570 Academic Word List For IELTSXanh Lè100% (1)
- 30-01-2014 Test Malik Asif Javaid AwanDokument4 Seiten30-01-2014 Test Malik Asif Javaid AwanDr-Usman Khan67% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Dha Prometric Feb-3 ShabeerDokument2 SeitenDha Prometric Feb-3 ShabeerDr-Usman KhanNoch keine Bewertungen
- Writing Task 1 1-8Dokument28 SeitenWriting Task 1 1-8Dr-Usman KhanNoch keine Bewertungen
- Dha Prometric Feb-3 ShabeerDokument2 SeitenDha Prometric Feb-3 ShabeerDr-Usman KhanNoch keine Bewertungen
- DHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDokument4 SeitenDHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDr-Usman Khan79% (14)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Good CommunicationDokument6 SeitenGood CommunicationKranthi KumarNoch keine Bewertungen
- The Drugs Act, 1976Dokument32 SeitenThe Drugs Act, 1976Dr-Usman KhanNoch keine Bewertungen
- Chemotheraphy and Its Side EffectsDokument2 SeitenChemotheraphy and Its Side EffectsALYSSA MAE RAPERNoch keine Bewertungen
- Pyrantel Dosage Guide With PrecautionsDokument1 SeitePyrantel Dosage Guide With PrecautionsMey KhNoch keine Bewertungen
- BCS Class PDFDokument14 SeitenBCS Class PDFdhimas11100% (1)
- Antiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionDokument22 SeitenAntiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionNaela RizqiNoch keine Bewertungen
- ChemotherapyDokument7 SeitenChemotherapyraecmyNoch keine Bewertungen
- RANITIDINE - Ranitidine Hydrochloride Injection, Solution: Page 1 of 9Dokument9 SeitenRANITIDINE - Ranitidine Hydrochloride Injection, Solution: Page 1 of 9Nur Syamsiah LaisaNoch keine Bewertungen
- Medicine Price List MPL Acute and Chronic November 2020Dokument123 SeitenMedicine Price List MPL Acute and Chronic November 2020karar hussainNoch keine Bewertungen
- 07.04.05 Venturi Face Mask PDFDokument2 Seiten07.04.05 Venturi Face Mask PDFRosintchi MirsalNoch keine Bewertungen
- Muscle Energy Techniquesto Correct Postural DysfunctionsDokument3 SeitenMuscle Energy Techniquesto Correct Postural DysfunctionsdasaNoch keine Bewertungen
- Maxolon Injection 5 MG / MLDokument1 SeiteMaxolon Injection 5 MG / MLJunaid IjazNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Moh Exam Prep MaterialDokument159 SeitenMoh Exam Prep MaterialAbid Ali Khan100% (1)
- Danger, Medicine, Fitness and Health VocabularyDokument4 SeitenDanger, Medicine, Fitness and Health VocabularyPhương ThảoNoch keine Bewertungen
- Pharmacy Board - Guidelines - Guidelines For Dispensing of MedicinesDokument19 SeitenPharmacy Board - Guidelines - Guidelines For Dispensing of MedicinesAnna WangNoch keine Bewertungen
- Bevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0Dokument6 SeitenBevacizumab Carboplatin Paclitaxel For Cervical Cancers CRP14GY017 v1.0andibarosNoch keine Bewertungen
- Classification Des MédicamentsDokument28 SeitenClassification Des MédicamentsGustyl KolinsNoch keine Bewertungen
- Walmart Drug ListDokument6 SeitenWalmart Drug ListShirley Pigott MDNoch keine Bewertungen
- Management of Severe Local Anaesthetic ToxicityDokument2 SeitenManagement of Severe Local Anaesthetic Toxicitymonir61Noch keine Bewertungen
- PharmacologyDokument236 SeitenPharmacologyyalahopa100% (2)
- Common Drugs - Med WardDokument1 SeiteCommon Drugs - Med WardRohannah D. MalawadNoch keine Bewertungen
- Nama Item AlkesDokument17 SeitenNama Item Alkesrian agustianNoch keine Bewertungen
- LM Database of Radiation OncologistsDokument17 SeitenLM Database of Radiation OncologistsNishant ChandraNoch keine Bewertungen
- Medication AdministrationDokument10 SeitenMedication AdministrationJemma NocalanNoch keine Bewertungen
- Studi Bioekivalensi Amoksisilin Generik Dan Dagang Menggunakan Matriks UrinDokument7 SeitenStudi Bioekivalensi Amoksisilin Generik Dan Dagang Menggunakan Matriks UrinEA12345aeNoch keine Bewertungen
- 1.application To Market A New DrugDokument4 Seiten1.application To Market A New DrugcardiacanesthesiaNoch keine Bewertungen
- (9781585286584 - ASHP® Injectable Drug Information™) Preliminary MaterialDokument24 Seiten(9781585286584 - ASHP® Injectable Drug Information™) Preliminary MaterialSathundorn NuntaNoch keine Bewertungen
- Stock 27072023 - ShareDokument80 SeitenStock 27072023 - ShareDanang WahyuNoch keine Bewertungen
- Anesthesia For Day-Care SurgeryDokument13 SeitenAnesthesia For Day-Care SurgeryMadhur AcharyaNoch keine Bewertungen
- Students Practical Training Report Project As Per PCI NormsDokument82 SeitenStudents Practical Training Report Project As Per PCI NormsAakif Anjum100% (1)
- Salinan Dari Jadwal KF Kedung CowekDokument47 SeitenSalinan Dari Jadwal KF Kedung Cowekdwikamaliyatissholehah94Noch keine Bewertungen
- TabletsDokument2 SeitenTabletsHector De VeraNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)