Das könnte Ihnen auch gefallen
- Bronchure PTSDDokument3 SeitenBronchure PTSDChristian LeepoNoch keine Bewertungen
- CH 46 Complications of AnaesthesiaDokument29 SeitenCH 46 Complications of AnaesthesiaChristian LeepoNoch keine Bewertungen
- CH 39 Anaesthesia and Diabetes MellitusDokument6 SeitenCH 39 Anaesthesia and Diabetes MellitusChristian LeepoNoch keine Bewertungen
- CH 21 Obstetric AnaesthesiaDokument39 SeitenCH 21 Obstetric AnaesthesiaChristian LeepoNoch keine Bewertungen
- CH 19 Spinal AnaesthesiaDokument29 SeitenCH 19 Spinal AnaesthesiaChristian Leepo100% (1)
- CH 13 Low Cost EquipmentDokument16 SeitenCH 13 Low Cost EquipmentChristian LeepoNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Daftar Obat Lasa & High AllertDokument4 SeitenDaftar Obat Lasa & High Allerttri tanayawatiNoch keine Bewertungen
- Mendelson SyndromeDokument6 SeitenMendelson SyndromeResa PutraNoch keine Bewertungen
- 9100C Urm - Ge AnesthesiaDokument174 Seiten9100C Urm - Ge AnesthesiaJohn Joseph LuNoch keine Bewertungen
- Resume of Intravenous Procaine Therapy PDFDokument6 SeitenResume of Intravenous Procaine Therapy PDFluanadumitruNoch keine Bewertungen
- Persistent Paralysis After Spinal Paresthesia PDFDokument6 SeitenPersistent Paralysis After Spinal Paresthesia PDFNadia Gina AnggrainiNoch keine Bewertungen
- Siyu 2Dokument4 SeitenSiyu 2siti nur asiahNoch keine Bewertungen
- Class X - CBSE Marking Scheme 2012 PDFDokument679 SeitenClass X - CBSE Marking Scheme 2012 PDFsreevalsan68Noch keine Bewertungen
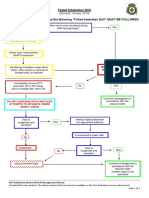
- Failed Intubation Drill Jan 10Dokument1 SeiteFailed Intubation Drill Jan 10Suni AbrahamNoch keine Bewertungen
- BRS General SurgeryDokument520 SeitenBRS General SurgeryWilliam Wiryawan100% (18)
- Effectiveness Injection Local Anesthesia Lignocaine2%Dokument1 SeiteEffectiveness Injection Local Anesthesia Lignocaine2%mdnajibkzmnNoch keine Bewertungen
- For Website All Questions PDFDokument26 SeitenFor Website All Questions PDFAyyaz HussainNoch keine Bewertungen
- G BehavGuide PDFDokument9 SeitenG BehavGuide PDFAzi Pertiwi HussainNoch keine Bewertungen
- Orif ReportDokument5 SeitenOrif ReportduypalaNoch keine Bewertungen
- Physiology of PainDokument75 SeitenPhysiology of PainJyoti RahejaNoch keine Bewertungen
- SRNA Orientation ChecklistDokument40 SeitenSRNA Orientation Checklistihtisham1Noch keine Bewertungen
- Nformation ACK: Specialty Doctor in Anaesthetics and Intensive Care Post Reference 415-MP499-21Dokument17 SeitenNformation ACK: Specialty Doctor in Anaesthetics and Intensive Care Post Reference 415-MP499-21Daniyal AzmatNoch keine Bewertungen
- SRMJResDentSci2296-8008867 221448Dokument4 SeitenSRMJResDentSci2296-8008867 221448Siddharth DhanarajNoch keine Bewertungen
- Effectiveness and Safety of Intravenous Sedation With Propofol in Non-Operating Room Anesthesia (NORA) For Dental Treatment in Uncooperative Paediatric PatientsDokument11 SeitenEffectiveness and Safety of Intravenous Sedation With Propofol in Non-Operating Room Anesthesia (NORA) For Dental Treatment in Uncooperative Paediatric PatientsharvardboyNoch keine Bewertungen
- Anesthetic Delivery SystemsDokument10 SeitenAnesthetic Delivery SystemsMichelle LindsayNoch keine Bewertungen
- Pharmacology: General Anaesthetic AgentsDokument65 SeitenPharmacology: General Anaesthetic AgentsSharifa DarayanNoch keine Bewertungen
- Case Log DefinitionsDokument6 SeitenCase Log DefinitionsSarah DNoch keine Bewertungen
- Anaesthesia For The Obese Patient: A. Wynn-Hebden and D.C. BouchDokument8 SeitenAnaesthesia For The Obese Patient: A. Wynn-Hebden and D.C. BouchdullzineaaNoch keine Bewertungen
- First QuizDokument6 SeitenFirst QuizCharlz ZipaganNoch keine Bewertungen
- NABH QI ListDokument9 SeitenNABH QI ListMangesh VirkarNoch keine Bewertungen
- EHE8-B5 User ManualDokument33 SeitenEHE8-B5 User ManualwilmerNoch keine Bewertungen
- ASA Neuroaxial in Parturient With Intracranial PathologyDokument16 SeitenASA Neuroaxial in Parturient With Intracranial PathologyKj BrionesNoch keine Bewertungen
- SSP Hospital Empanelment Criteria FinalDokument19 SeitenSSP Hospital Empanelment Criteria FinalEngr Saba AfzalNoch keine Bewertungen
- University of Bahrain: Quality Assurance and Accreditation CenterDokument6 SeitenUniversity of Bahrain: Quality Assurance and Accreditation Centerrehab ebraheemNoch keine Bewertungen
- Local AnestheticsDokument35 SeitenLocal AnestheticsNia NaNa Try FaithfulNoch keine Bewertungen
- Siare Perseo - Service ManualDokument55 SeitenSiare Perseo - Service ManualsolcarwxNoch keine Bewertungen