Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 3-23-22 Sa Gamot Na Abot Kaya, Sakit Makakaya 3Dokument21 Seiten3-23-22 Sa Gamot Na Abot Kaya, Sakit Makakaya 3Rachelle Joy G. Bugatan100% (1)
- Trade Name Generic Name Group: TetracyclinesDokument11 SeitenTrade Name Generic Name Group: Tetracyclinesmisfer72Noch keine Bewertungen
- Icf Pri P2 414 PDFDokument17 SeitenIcf Pri P2 414 PDFMichael Forest-dNoch keine Bewertungen
- GN BN Part IDokument2 SeitenGN BN Part ICarla Flor LosiñadaNoch keine Bewertungen
- Hypertension and Cognitive ImpairmentDokument3 SeitenHypertension and Cognitive ImpairmentMekonninNoch keine Bewertungen
- HW3 PharmacologyDokument8 SeitenHW3 PharmacologyMICHAEL GABRIEL JIMENEZNoch keine Bewertungen
- Platinum Formulary 2016Dokument61 SeitenPlatinum Formulary 2016jNoch keine Bewertungen
- Perindopril and Indopamide Assay by UPLCDokument6 SeitenPerindopril and Indopamide Assay by UPLCAmarNoch keine Bewertungen
- ASCOT Hypertension StudyDokument12 SeitenASCOT Hypertension StudyAnonymous NeRC5JYiSNoch keine Bewertungen
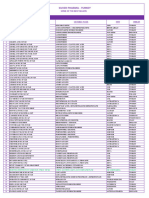
- Genericsking Trading Inc Generics Medicines Wholesale - NewDokument10 SeitenGenericsking Trading Inc Generics Medicines Wholesale - NewCrystal NgNoch keine Bewertungen
- Some of The Best Sellers SILVER PHARMA TURKEYDokument3 SeitenSome of The Best Sellers SILVER PHARMA TURKEYArchil PochkhuaNoch keine Bewertungen
- 3 ACC Prevention Blood PressureDokument69 Seiten3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- Switching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilDokument2 SeitenSwitching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilGlory Claudia KarundengNoch keine Bewertungen
- Triplixam 10mg - 2-5mg - 10mg Film Coated Tablets (Perindopril Arginine - Indapamide - Amlodipine)Dokument8 SeitenTriplixam 10mg - 2-5mg - 10mg Film Coated Tablets (Perindopril Arginine - Indapamide - Amlodipine)Sze Wei TanNoch keine Bewertungen
- Medicines & Supplies: FebruaryDokument85 SeitenMedicines & Supplies: FebruaryPharmacy DeamhiNoch keine Bewertungen
- Practical MCQ Question For 4-YearDokument39 SeitenPractical MCQ Question For 4-Yearkhuzaima9100% (2)
- Cover Syl TabDokument14 SeitenCover Syl TabTEte TEteNoch keine Bewertungen
- Summary of Product Characteristics, Labelling and Package LeafletDokument29 SeitenSummary of Product Characteristics, Labelling and Package LeafletImmanuel PurbaNoch keine Bewertungen
- Hospital Formulary ADokument13 SeitenHospital Formulary Alesliemaebarlaan03Noch keine Bewertungen
- Medis Dossier Portfolio Oct 2015 PDFDokument8 SeitenMedis Dossier Portfolio Oct 2015 PDFiyad.alsabiNoch keine Bewertungen
- Endocrinology and DiabetesDokument29 SeitenEndocrinology and DiabetesCarlos HernándezNoch keine Bewertungen
- Coveram: What Is in This LeafletDokument5 SeitenCoveram: What Is in This LeafletLim Yan WeiNoch keine Bewertungen
- L A S A Lasa: Action To Be TakenDokument9 SeitenL A S A Lasa: Action To Be TakenKok Hui DiongNoch keine Bewertungen
- VXL-List of Pharma Products (Domestic and Export)Dokument10 SeitenVXL-List of Pharma Products (Domestic and Export)Singh PushpanjaliNoch keine Bewertungen
- Finished Copy of Drug Formulary 29 MAy 2014 With PicturesDokument89 SeitenFinished Copy of Drug Formulary 29 MAy 2014 With Picturesshameena1234Noch keine Bewertungen
- Europa Trial PDFDokument2 SeitenEuropa Trial PDFShawnNoch keine Bewertungen
- MRP Omnibus (ENG) V.finalDokument13 SeitenMRP Omnibus (ENG) V.finaladharra crystal dorin100% (1)
- Drug StudyDokument2 SeitenDrug StudyAnne Nicole ObispoNoch keine Bewertungen
- Fi H 0840 004 ParDokument16 SeitenFi H 0840 004 ParNathaniel Roi BalbarinoNoch keine Bewertungen
- CS ReportDokument135 SeitenCS Reporthindupur dispensaryNoch keine Bewertungen