Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Kuliah Biokimia-Imunokimia FK UNDIPDokument19 SeitenKuliah Biokimia-Imunokimia FK UNDIPPutri HapsariNoch keine Bewertungen
- Clsi Ila02 ADokument36 SeitenClsi Ila02 ACristian Gutiérrez VeraNoch keine Bewertungen
- Literature Review On Immunization in NigeriaDokument13 SeitenLiterature Review On Immunization in Nigeriaaflsigfek100% (1)
- Module 5 - Formative Assessment 10 - NCM 112 CARE OF CLIENTS WITH PROBLEMS IN OXYGFENATION FLUDokument9 SeitenModule 5 - Formative Assessment 10 - NCM 112 CARE OF CLIENTS WITH PROBLEMS IN OXYGFENATION FLUDharylle CariñoNoch keine Bewertungen
- Chicken Pox PresentationDokument14 SeitenChicken Pox Presentationnur syafiqah kamaruzaman100% (3)
- Viral MeningitisDokument4 SeitenViral MeningitisLucky PuspitasariNoch keine Bewertungen
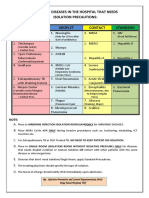
- Common Hospital Diseases Requiring Isolation PrecautionsDokument1 SeiteCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNoch keine Bewertungen
- Clsi 2012Dokument50 SeitenClsi 2012niluh suwasanti100% (1)
- Topic Presentation Henoch-Schonlein Purpura (HSP) : Name: Sweta Jaanvhi Raj S160258 DATE: 16/09/2020Dokument26 SeitenTopic Presentation Henoch-Schonlein Purpura (HSP) : Name: Sweta Jaanvhi Raj S160258 DATE: 16/09/2020Alusio Navosailagi VUNIIVINoch keine Bewertungen
- Ampiginosa 1Dokument5 SeitenAmpiginosa 1Juan BianchiNoch keine Bewertungen
- 2009432Dokument32 Seiten2009432Luis Alberto Letona QuispeNoch keine Bewertungen
- COVID 19 Potential Impact On Asthma PatientsDokument73 SeitenCOVID 19 Potential Impact On Asthma PatientsWahyu PurnamaNoch keine Bewertungen
- NCP Burn Risk InfectionDokument1 SeiteNCP Burn Risk InfectionBraingie Racho50% (4)
- 14 HF-Limfoma GI TractDokument27 Seiten14 HF-Limfoma GI TractNur akilaNoch keine Bewertungen
- Alinity Toxo MDokument7 SeitenAlinity Toxo MLoloNoch keine Bewertungen
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDokument52 SeitenCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaNoch keine Bewertungen
- Bone Marrow Niches HSC FatesDokument1 SeiteBone Marrow Niches HSC FatesAdelina PirvanNoch keine Bewertungen
- Rheumatic FeverDokument16 SeitenRheumatic Feversteve benNoch keine Bewertungen
- Pathogen Research AssignmentDokument2 SeitenPathogen Research AssignmentDeven BaliNoch keine Bewertungen
- Peer Review HatchDokument3 SeitenPeer Review Hatchapi-680921549Noch keine Bewertungen
- Brain Abscess (MEDSURG)Dokument3 SeitenBrain Abscess (MEDSURG)Yessamin Paith RoderosNoch keine Bewertungen
- BronchiectasisDokument16 SeitenBronchiectasisRaras RavenclawwNoch keine Bewertungen
- Treatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionDokument24 SeitenTreatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionMuhammad Farras Razin PerdanaNoch keine Bewertungen
- Case Study HIV With DiarrheaDokument29 SeitenCase Study HIV With DiarrheaMatin Ahmad Khan100% (1)
- Gapuz Communicable Disease NursingDokument46 SeitenGapuz Communicable Disease NursingBJ DUQUESANoch keine Bewertungen
- Hazardous Ingredients of HPV Vaccines Increase Risk To Young People#@Dokument19 SeitenHazardous Ingredients of HPV Vaccines Increase Risk To Young People#@Dan TudorNoch keine Bewertungen
- Per-Pl 206Dokument266 SeitenPer-Pl 206Wan YusufNoch keine Bewertungen
- Pro-Inflammatory Effects of Hypoglycemia in Humans With or Without DiabetesDokument32 SeitenPro-Inflammatory Effects of Hypoglycemia in Humans With or Without Diabetestitin setya ningsihNoch keine Bewertungen
- Homologous or Heterologous Booster of Inactivated Vaccine Reduces Sars-Cov-2 Omicron Variant Escape From Neutralizing AntibodiesDokument12 SeitenHomologous or Heterologous Booster of Inactivated Vaccine Reduces Sars-Cov-2 Omicron Variant Escape From Neutralizing AntibodiesSariSyahruniNoch keine Bewertungen
- Introduction To Serology - Immunology, HSV & H.pyloriDokument37 SeitenIntroduction To Serology - Immunology, HSV & H.pyloritriaclaresiaNoch keine Bewertungen