Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mol Bio Classics PDFDokument11 SeitenMol Bio Classics PDFreoloxNoch keine Bewertungen
- The Human Genome - FinalDokument27 SeitenThe Human Genome - FinalAbhi SachdevNoch keine Bewertungen
- Botany XI Chapter1 Biological ClassificationDokument68 SeitenBotany XI Chapter1 Biological ClassificationSDO BSNL NALAGARHNoch keine Bewertungen
- Introduction To Microbial Pathogenicity: Presented byDokument11 SeitenIntroduction To Microbial Pathogenicity: Presented byAy GlassesNoch keine Bewertungen
- Virology Micro D&R AgamDokument142 SeitenVirology Micro D&R AgamNirosha ArulNoch keine Bewertungen
- Wang 2009Dokument8 SeitenWang 2009biborka0501Noch keine Bewertungen
- Gram Negative Aerobic and Facultative RodsDokument53 SeitenGram Negative Aerobic and Facultative RodsChatie PipitNoch keine Bewertungen
- MCB502 2020 Exam #1Dokument9 SeitenMCB502 2020 Exam #1Cameron KeetonNoch keine Bewertungen
- Pathogen Frequencies (CFAD Ch. 17) - Zapper Wiki - FandomDokument14 SeitenPathogen Frequencies (CFAD Ch. 17) - Zapper Wiki - FandomluisNoch keine Bewertungen
- Rubella Virus Info 1Dokument5 SeitenRubella Virus Info 1Michael W.100% (1)
- Graphene Oxide and CovidDokument15 SeitenGraphene Oxide and CovidaliaNoch keine Bewertungen
- Media Farmasi P.issn 0216-2083 E.issn 2622-0962 Vol. XV No. 1, April 2019Dokument6 SeitenMedia Farmasi P.issn 0216-2083 E.issn 2622-0962 Vol. XV No. 1, April 2019Ivanda PrilsciliaNoch keine Bewertungen
- Histology: A Text and Atlas: January 1995Dokument3 SeitenHistology: A Text and Atlas: January 1995Roxana RaduNoch keine Bewertungen
- TGA Letter of Demand - 4 July 2023Dokument30 SeitenTGA Letter of Demand - 4 July 2023Tim BrownNoch keine Bewertungen
- Introduction To Bioprocessing NewDokument58 SeitenIntroduction To Bioprocessing NewAmit SinghNoch keine Bewertungen
- Ivy Jean MartinezDokument11 SeitenIvy Jean MartinezmarjmarjNoch keine Bewertungen
- Btech Complementation Test RII LocusDokument38 SeitenBtech Complementation Test RII LocusTannishtha DattaNoch keine Bewertungen
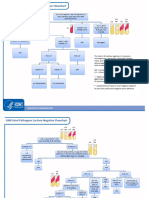
- GNR Stool Pathogens Lactose Negative FlowchartDokument2 SeitenGNR Stool Pathogens Lactose Negative FlowchartKeithNoch keine Bewertungen
- XI Bio Chapter 02 Biological ClassificationDokument13 SeitenXI Bio Chapter 02 Biological ClassificationSanaNoch keine Bewertungen
- Paper 2 November 2001Dokument5 SeitenPaper 2 November 2001MSHNoch keine Bewertungen
- Chapter 8Dokument53 SeitenChapter 8contactrafiakhuramNoch keine Bewertungen
- IMY Unit 1, Sub Unit 1.1Dokument11 SeitenIMY Unit 1, Sub Unit 1.1fdvfsgffefNoch keine Bewertungen
- European S3-Guidelines On The Systemic Treatment of PsoriasisDokument208 SeitenEuropean S3-Guidelines On The Systemic Treatment of Psoriasisghitza80Noch keine Bewertungen
- Acquired Hemolytic AnemiaDokument48 SeitenAcquired Hemolytic AnemiaJeena RajNoch keine Bewertungen
- STS Midterms ReviewerDokument19 SeitenSTS Midterms ReviewerJaela Rebekah TotañesNoch keine Bewertungen
- Lecture - Week 3 (Natural Immunity & Complement System)Dokument5 SeitenLecture - Week 3 (Natural Immunity & Complement System)rennel ybarolaNoch keine Bewertungen
- Cell Biology Pollard 2e PDFDokument927 SeitenCell Biology Pollard 2e PDFМарина Попозогло86% (7)
- Nitroimidazole Wps OfficeDokument10 SeitenNitroimidazole Wps OfficeCamelle DiniayNoch keine Bewertungen
- The Genexpert System: Designed To Grow: A Modular Platform ApproachDokument2 SeitenThe Genexpert System: Designed To Grow: A Modular Platform Approachbashaar ahmedNoch keine Bewertungen
- Magnetic Pulse Therapy and Rife HealingDokument9 SeitenMagnetic Pulse Therapy and Rife HealingHaSophim88% (8)