Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Brenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuDokument4 SeitenBrenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuJim Dominguez RosalesNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- EMQ Samples MicrobiologyDokument5 SeitenEMQ Samples MicrobiologyHugh JacobsNoch keine Bewertungen
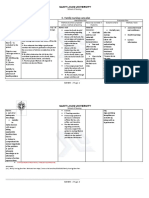
- C. Family Nursing Care Plan: Saint Louis UniversityDokument2 SeitenC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- 101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinDokument17 Seiten101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinFilipeCarvalho100% (7)
- KINESIOTHERAPHYDokument40 SeitenKINESIOTHERAPHYJeyarajasekar TtrNoch keine Bewertungen
- Jama Sanders 2020 RV 200005Dokument13 SeitenJama Sanders 2020 RV 200005Juan Carlos PabonNoch keine Bewertungen
- Handbook of TransplantDokument496 SeitenHandbook of Transplantfa7mi77Noch keine Bewertungen
- Markers of and Risk Factors For The Development andDokument24 SeitenMarkers of and Risk Factors For The Development andJim Dominguez RosalesNoch keine Bewertungen
- Eplerenone and Atrial Fibrillation in Mild Systolic Heart FailureDokument6 SeitenEplerenone and Atrial Fibrillation in Mild Systolic Heart FailureJim Dominguez RosalesNoch keine Bewertungen
- Clinical Challenges in Diagnosis and Management of Diabetic PDFDokument19 SeitenClinical Challenges in Diagnosis and Management of Diabetic PDFJim Dominguez RosalesNoch keine Bewertungen
- Fod CentralDokument19 SeitenFod CentralJim Dominguez RosalesNoch keine Bewertungen
- Syndrome CardiorenalDokument13 SeitenSyndrome CardiorenalJim Dominguez RosalesNoch keine Bewertungen
- VSG y PCRDokument6 SeitenVSG y PCRJim Dominguez RosalesNoch keine Bewertungen
- Acido Base CompensacionDokument4 SeitenAcido Base CompensacionJim Dominguez RosalesNoch keine Bewertungen
- Dy NamedDokument29 SeitenDy NamedJim Dominguez RosalesNoch keine Bewertungen
- European Best Practice Guidelines On Vascular Access 2007Dokument30 SeitenEuropean Best Practice Guidelines On Vascular Access 2007Jim Dominguez RosalesNoch keine Bewertungen
- Dia Care-2014 - S14-80Dokument67 SeitenDia Care-2014 - S14-80Jim Dominguez RosalesNoch keine Bewertungen
- Mayo Clin ProC - REVISONDokument13 SeitenMayo Clin ProC - REVISONJim Dominguez RosalesNoch keine Bewertungen
- 1970 - Zuger Vs Money-A Critical Review of The Evidence From HermaphroditismDokument20 Seiten1970 - Zuger Vs Money-A Critical Review of The Evidence From HermaphroditismRafael FredaNoch keine Bewertungen
- What Is Rejection Sensitive DysphoriaDokument3 SeitenWhat Is Rejection Sensitive DysphoriaDomingo Ignacio100% (3)
- Effects of Activator and High Pull Headgear Combination Therapy PDFDokument9 SeitenEffects of Activator and High Pull Headgear Combination Therapy PDFDilesh PradhanNoch keine Bewertungen
- Paediatric Respiratory Disease: Parenchymal DiseasesDokument95 SeitenPaediatric Respiratory Disease: Parenchymal DiseasesAndrei Ian100% (1)
- Prevalence of Overhang Interproximal Amalgam RestorationsDokument4 SeitenPrevalence of Overhang Interproximal Amalgam RestorationsNaji Z. ArandiNoch keine Bewertungen
- Assignment and Delegation Guidelines: For Registered Nurses and Licensed Practical NursesDokument20 SeitenAssignment and Delegation Guidelines: For Registered Nurses and Licensed Practical Nursesanna regarNoch keine Bewertungen
- Lyme DiseaseDokument133 SeitenLyme Diseaseernestval100% (3)
- Temos Dental Standards Accredited by ISQua/IEEA Four New Accreditation Options Designed by Dentists For DentistsDokument3 SeitenTemos Dental Standards Accredited by ISQua/IEEA Four New Accreditation Options Designed by Dentists For DentistsPR.comNoch keine Bewertungen
- Benefits of Medical Expert SystemsDokument27 SeitenBenefits of Medical Expert Systemsrobertxxx100% (1)
- Alzehimer GuiaDokument9 SeitenAlzehimer GuiaAlejandro PiscitelliNoch keine Bewertungen
- Complications-Hypoglycemia Ada PDFDokument68 SeitenComplications-Hypoglycemia Ada PDFjorgefjdNoch keine Bewertungen
- Sonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFDokument15 SeitenSonography of Normal and Abnormal Thyroid and Parathyroid Glands PDFJheyson Javier Barrios PereiraNoch keine Bewertungen
- AdenoidsDokument8 SeitenAdenoidsUjjawalShriwastavNoch keine Bewertungen
- NCP 1activity Intolerance N C P BY BHERU LALDokument1 SeiteNCP 1activity Intolerance N C P BY BHERU LALBheru LalNoch keine Bewertungen
- RA 7305 The Magna Carta of Public Health WorkersDokument11 SeitenRA 7305 The Magna Carta of Public Health WorkersJessie Espino Vega100% (1)
- Chronic Kidney DiseaseDokument12 SeitenChronic Kidney DiseaseRoseben SomidoNoch keine Bewertungen
- Free Report-Smoking CessationDokument5 SeitenFree Report-Smoking CessationdapextilburyNoch keine Bewertungen
- Hypersensitivity: Dr. Amit Makkar, Sudha Rustagi Dental CollegeDokument117 SeitenHypersensitivity: Dr. Amit Makkar, Sudha Rustagi Dental Collegeamitscribd1Noch keine Bewertungen
- The Cost of PainDokument121 SeitenThe Cost of PainDavid IrelandNoch keine Bewertungen
- Chronic Care ManagementDokument8 SeitenChronic Care ManagementJubyNoch keine Bewertungen
- AntihistaminesDokument2 SeitenAntihistaminesmercywicherNoch keine Bewertungen
- CareerAssessmentQuestionnaire v8!1!14Dokument1 SeiteCareerAssessmentQuestionnaire v8!1!14Alain CheryNoch keine Bewertungen
- Kruszewski 2nd Amended Complaint FILED 12-28-05Dokument12 SeitenKruszewski 2nd Amended Complaint FILED 12-28-05Art Levine, Mental Health Inc.Noch keine Bewertungen
- Tumori Tesuturi MoiDokument123 SeitenTumori Tesuturi MoiOana BarbuNoch keine Bewertungen
- Tracy Terrones Resume 1Dokument2 SeitenTracy Terrones Resume 1api-315217520Noch keine Bewertungen
- Multiple Atrophy System (MSA) Trust Caregiver's GuideDokument11 SeitenMultiple Atrophy System (MSA) Trust Caregiver's GuideThe Multiple System Atrophy CoalitionNoch keine Bewertungen