DOI: 10.5958/j.2319-5886.3.1.
003
International Journal of Medical Research & Health Sciences
www.ijmrhs.com Volume 3 Issue 1 (Jan- Mar)
Received: 6 Sep 2013
th
Coden: IJMRHS
th
Copyright @2013
ISSN: 2319-5886
Revised: 9 Oct 2013
Accepted: 4th Nov 2013
Research article
A STUDY ON CHANGES IN SERUM GGT AND MAGNESIUM LEVEL IN ALCOHOLIC LIVER DISEASE *Gandhi Paulin A1, Sendhav Sandip S2, Sanghani Hiren I2, Patel Arpita P3
1 2
Tutor, Departments of Biochemistry, G.C.S. Medical College, Ahmedabad, Gujarat, India Senior Resident, Departments of Biochemistry, B. J. Medical College & Civil Hospital, Ahmedabad, Gujarat 3 Junior Lecturer, Departments of Biochemistry, N.H.L. Medical College, Ahmedabad, Gujarat, India *Corresponding author email: pautalk@gmail.com ABSRACT Aims: A study on changes in Serum GGT and Magnesium level in Alcoholic Liver Disease. Material and Methods: Serum GGT and Serum Mg++ were estimated with the help of commercially available kit in patients of Alcoholic Liver Disease (n=50) and Normal Individuals (n=50) on fully automated biochemistry analyzer Erba XL-640. Results: Serum GGT level was found significantly higher (P< 0.01) in Alcoholic patients as compared to healthy non-alcoholics. Moreover Serum Mg++ was found significantly lower (P< 0.01) in Alcoholic Liver Disease as compare to normal Individuals. In addition to that there is significant inverse correlation (r= - 0.553) between serum GGT and Mg++ in study group. Conclusions: None of the individual tests of conventional liver function tests are of much importance in diagnosis of liver disease; however when many of the liver function tests are abnormal at the same time, liver disease is the most probable diagnosis. Data of the present study clearly conclude that serum GGT activity along with serum Mg++ status can be useful marker for alcoholic liver disease. Keywords: Gamma Glutamyl Transferase, Magnesium, Alcoholic Liver Disease INTRODUCTION Excessive alcohol consumption and consequent medical disorders are considerable problems in our countries which causes a wide variety of medical and social problems1. It is estimated that only 20-50 % of patients with alcoholism are actually identified in health care and thus more reliable and accurate methods are urgently needed. There is no exact clinical finding or symptom clinical setting that can detect alcohol abuse in its early phase. So there are some biochemical substances in the body that can indicate the presence or progress of a condition or any genetic predisposition toward it, are called Biomarkers 2 which may detect excessive drinking and evaluate the extent of the resultant tissue damage. Gamma-glutamyl transferase (GGT) is a membranebound glycoprotein enzyme which catalyzes the Gandhi et al., transfer of the gamma-glutamyl moiety of glutathione to various peptide acceptors. Chronic ethanol consumption induces a rise in serum GGT, and it has therefore been widely used as an index of excessive ethanol intake 3-4. Its sensitivity varied from 15 to 85% in previous studies8-10. Recent work by comparing alcoholic group with normal control group which emphasis on important factor serum GGT activities which can increase in case of alcoholics 5-6. Magnesium (Mg++) a ubiquitous element, involve in membrane stabilization, ion transport, and Ca++ channel activity, cofactor for more than 300 enzymes 7 , may get depleted by several mechanisms associated with alcoholism like magnesium deficiency, including urinary Mg++ wastage, malnutrition, gastrointestinal losses, phosphate deficiency, acidosis/alkalosis, vitamin D deficiency etc.
12
Int J Med Res Health Sci. 2014;3(1):12-15
This work was aimed at investigating the diagnostic value of serum GGT level and Serum Mg++ level and correlation of serum GGT and Mg in the evaluation of chronic alcoholic liver disease. MATERIALS AND METHODS In the present cross-sectional study, 50 cases of Alcoholic liver disease and 50 normal individuals were selected from OPD and various clinical wards of B.J. Medical College and Civil Hospital, Ahmadabad, Gujarat during the period of April 2010 to December 2012. The study was approved by the BJ Medical college, Ahmadabad and inform consent form was obtained form the all participants. All patients were primarily evaluated by clinical examination and then confirmed by investigations for liver involvement due to alcoholism. In study group (n=50), we have included male patients between age of 20 60 years, BMI 30 kg/m 2, alcohol consumption for at least last 5 years with clinical evidence of alcoholic liver dysfunction. In control group (n=50), we have included normal healthy individuals having same age RESULTS
and sex. Exclusion criteria: Age < 20 or >60 years, Athletes, Clinical Evidence of current illness, Clinical evidence of any chronic infection, Smoking had not been allowed 1 hour prior to sampling, Protein energy malnutrition, Post operative patient, Patient taking anticonvulsant therapy (Benzodiazepines, 2 Phenobarbitone), BMI > 30 kg/m , Serum Bilirubin level > 20 mg/dL. Venous blood was collected in clot activator serum vacutte from all the participants. Serum was separated and analyzed for GGT, Mg on fully Auto Analyzer Erba XL-640 at Biochemistry Section. Serum GGT was analyzed by carboxy substrate8 method and serum Mg was analyzed by calmagite method9 with commercially available ready to use reagent kits. Numerical variables are reported in terms of mean and standard deviation. Comparison between two groups is made with the Mann-Whitney test 10. Correlations were calculated with pearson product moment correlation coefficient by using graphpad prism version 3.03 statistical software.
Table 1: Comparison of Serum GGT and Magnesium in Alcoholic Liver Disease and Normal Individual
Parameter
GGT Magnesium
Group-2 (Control Biological Group) Reference Interval n=50 Mean SD Mean SD 10-50 U/L 101.04 52.2 42.02 12.82 1.6 3.0 mg/dL 1.50 0.49 2.03 0.36 *P< 0.01: highly significant difference between two groups
3.5 3 Magnesium(mg/dL) 2.5 2 1.5 1 0.5 0 0 100
Group-1(ALD Patients) n=50
Significance P value P<0.01* P<0.01*
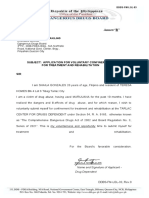
In this study we measured Serum activity of Gamma Glutamyl Transferase and Magnesium in both groups. There is highly significant difference observed in between study group and control group. Correlation between serum GGT and Magnesium level in alcoholic liver disease and normal individual during observation significant inverse correlation (r= - 0.533, P<0.01) was found in alcoholic patients whereas it was not significant in normal individual (r= 0.031, P>0.05).
Graph 1: Study Group
200
300
GGT (U/L) Fig 1; Correlation of serum GGT with magnesium in Study group
13
Gandhi et al., Int J Med Res Health Sci. 2014;3(1):12-15
Graph 2: Control Group
3.5 Magnesium (mg/dL) 3 2.5 2 1.5 1 0.5 0 0 20 40 60 80 100 GGT ( U/L) Fig 2: Correlation of serum GGT with magnesium in control group
DISCUSSION Liver serves many important biological functions to sustain life, so early diagnosis of liver involvement is of utmost priority to prevent life threatening complications. Over past decade a large number of new laboratory markers have emerged for alcohol abuse. One of these is Gamma Glutamyl Transferase. In order to assess its usefulness, I have studied Serum GGT level and Serum Magnesium in 50 patients of alcoholic liver disease and 50 normal individual. I have tried to match control with the disease population as far as possible. Glutamyl transpeptidase (GT) is an enzyme produced in the bile duct. It is induced by alcohol and its serum activity may be increased in heavy drinkers even in the absence of liver damage or inflammation. In this study the serum GT levels were markedly increased in alcoholic patients (P<0.01). The GGT activity in serum increases after induction of the enzyme, and the possibility of parenchymal damage should always be considered. The elevation of GT alone with no other liver function test abnormalities often results from induction by alcohol 11. The results of present study are correlate well with earlier studies by B. Usharani et al 2012 12, Turecky L et al. 2006 7, Subir kumar Das et al 2005 13 etc. Chronic alcohol abuse also causes primary malnutrition by insufficient dietary magnesium intake. Moreover, as the cause of secondary malnutrition chronic ethanol intake leads to functional and structural disorders in the gastrointestinal tract that result from its direct action Gandhi et al.,
on the gastrointestinal tract and damage to the liver and pancreas. In also affects the magnesium transport mechanisms in the plasma membrane, either directly (alcohol-related modification of the phospholipid environment or acetaldehyde-protein interaction) or indirectly (via the decrease in cellular ATP content).One of the major reasons for ethanolinduced hypomagnesaemia in alcohol abusers is increased urinary magnesium excretion due to damage to the renal proximal tubules and the Henle loop directly induced by ethanol 15-17. These study is also supported by data of previous studies Elisaf M. et al 1995 18 and Virginija Stasiukynien et al 2002 19. It is concluded from the present study that the estimation of serum GGT can be useful and more cost-effective in diagnosing alcoholic liver diseases as it significantly rises in alcoholic liver disease. Moreover, serum Mg can also be used as a marker of chronic alcoholic liver disease along with serum GGT as they have significant correlation in alcoholic liver disease. CONCLUSION
It is concluded from the present study that the estimation of serum GGT can be useful and more cost-effective in diagnosing alcoholic liver diseases as it significantly rises in alcoholic liver disease. Moreover, serum Mg can also be used as a marker of chronic alcoholic liver disease along with serum GGT as they have significant correlation in alcoholic liver disease.
REFERENCES 1. Room R, Babor T, Rehm, J. Alcohol and public health. Lancet 2005; 365: 51930. 2. Peterson K. Biomarkers for alcohol use and abuse: A summary. Alcohol Res Health 20042005; 28(1):30-37. 3. Zein M, Discombe G. Serum gamma-glutamyl transpeptidase as a diagnostic aid. The Lancet 1970; 296: 74850. 4. Gogoi JB, Tyagi PK, Amit Singh. Study of serum gamma glutamyl transferase as a diagnostic marker in alcoholic hepatitis. IOSR Journal of Pharmacy (IOSRPHR) 2012; 2; 69-71. 5. Peters TJ, Cook CC. Obesity as a cause of falsepositive alcohol misuse laboratory
14
Int J Med Res Health Sci. 2014;3(1):12-15
investigations. Addiction Biology 2002; 7:443 46. 6. Katri Puukka. Gamma-glutamyl Transferase As a Marker of Alcohol Abuse: Effects of Moderate Drinking, Obesity & Increasing Age on Reference Intervals, University of Tampere, Medical School Seinajoki Central Hospital, Department of Laboratory Medicine and Medical Research Unit, Finland, 2007: pp 15. 7. Turecky L, Kupcova V, Szantova M. Serum magnesium levels in patients with alcoholic and non-alcoholic fatty liver. Bratisl Lek Listy. 2006; 107(3):58-61.
chronic alcoholic patients during withdrawal. Medicina 2002; 38:892-95.
alcohol
8. Bergmeyer H-U, Horder M, Rej R. IFCC methods for the measurement of catalytic concentrations of enzymes, J. Clin. Chem. Clin Biochem. 1986; 24: 497-510. 9. Gindler E. Colorimetric Determination With Bound "Calmagite" of. Magnesium in Human Blood Serum. Clin. Chem.1971; 17: 662.
10. Rosie Shier. Statistics:2.3 The Mann-Whitney U Test. Mathematics learning support center 2004:1-5. 11. Keeffe EB, Sunderland MC, Gabourel JD. Serum gamma-glutamyl transpeptidase activity in patients receiving chronic phenytoin therapy.Dig Dis Sci. 1986; 31(10): 1056-61. 12. Usharani B, Vennila R, Nalini N. Biochemical changes in Alcoholics: A case control study. International Journal of Research in Pharmaceutical and Biomedical Sciences 2012; 3: 201-05. 13. Subir Kumar Das, Prasunpriya Nayak, Vasudevan DM. Biochemical markers for alcohol consumption. IJCB 2005, 20(1): 35-42 14. Kocur J. Concentration of bioelements in alcohol dependent patients. Biul.Magnezol. 1997; 2: 239. 15. Elisaf M, Merkooropoulos M. Pathogenetic mechanisms of hypomagnesaemia in alcoholic patients. J. Trace Elem. Med. Biol. 1996; 9: 210. 16. Vormann J. Magnesium: nutrition and metabolism. Mol. Aspects Med.2003; 24: 27. 17. Elisaf M, Merkouropoulos M, Tsianos EV. Pathogenetic mechanisms of hypomagnesemia in alcoholic patients. J Trace Elem Med Biol 1995; 9: 210-14. 18. Virginija Stasiukynien. Blood plasma potassium, sodium and magnesium levels in
15
Gandhi et al., Int J Med Res Health Sci. 2014;3(1):12-15
Das könnte Ihnen auch gefallen
- Ijmrhs Vol 4 Issue 3Dokument263 SeitenIjmrhs Vol 4 Issue 3editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 1 Issue 1Dokument257 SeitenIjmrhs Vol 1 Issue 1editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 3 Issue 2Dokument281 SeitenIjmrhs Vol 3 Issue 2editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 3 Issue 4Dokument294 SeitenIjmrhs Vol 3 Issue 4editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 3 Issue 3Dokument271 SeitenIjmrhs Vol 3 Issue 3editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 4 Issue 2Dokument219 SeitenIjmrhs Vol 4 Issue 2editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 4 Issue 4Dokument193 SeitenIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 3 Issue 1Dokument228 SeitenIjmrhs Vol 3 Issue 1editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 2 Issue 2Dokument197 SeitenIjmrhs Vol 2 Issue 2editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 1 Issue 1Dokument257 SeitenIjmrhs Vol 1 Issue 1editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 2 Issue 4Dokument321 SeitenIjmrhs Vol 2 Issue 4editorijmrhsNoch keine Bewertungen
- Ijmrhs Vol 2 Issue 1Dokument110 SeitenIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- Ijmrhs Vol 2 Issue 3Dokument399 SeitenIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- 47serban Turliuc EtalDokument4 Seiten47serban Turliuc EtaleditorijmrhsNoch keine Bewertungen
- 41anurag EtalDokument2 Seiten41anurag EtaleditorijmrhsNoch keine Bewertungen
- 48 MakrandDokument2 Seiten48 MakrandeditorijmrhsNoch keine Bewertungen
- 45mohit EtalDokument4 Seiten45mohit EtaleditorijmrhsNoch keine Bewertungen
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDokument2 SeitenRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsNoch keine Bewertungen
- 38vaishnavi EtalDokument3 Seiten38vaishnavi EtaleditorijmrhsNoch keine Bewertungen
- 43chaitali EtalDokument3 Seiten43chaitali EtaleditorijmrhsNoch keine Bewertungen
- 40vedant EtalDokument4 Seiten40vedant EtaleditorijmrhsNoch keine Bewertungen
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDokument3 SeitenWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsNoch keine Bewertungen
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDokument5 SeitenPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsNoch keine Bewertungen
- 35krishnasamy EtalDokument1 Seite35krishnasamy EtaleditorijmrhsNoch keine Bewertungen
- 33 Prabu RamDokument5 Seiten33 Prabu RameditorijmrhsNoch keine Bewertungen
- 36rashmipal EtalDokument6 Seiten36rashmipal EtaleditorijmrhsNoch keine Bewertungen
- 37poflee EtalDokument3 Seiten37poflee EtaleditorijmrhsNoch keine Bewertungen
- 34tupe EtalDokument5 Seiten34tupe EtaleditorijmrhsNoch keine Bewertungen
- 32bheemprasad EtalDokument3 Seiten32bheemprasad EtaleditorijmrhsNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Endometriosis: Epidemiology, Diagnosis and Clinical ManagementDokument9 SeitenEndometriosis: Epidemiology, Diagnosis and Clinical ManagementRubiahSheBiachNoch keine Bewertungen
- Narcotics Controlled Drugs TableDokument4 SeitenNarcotics Controlled Drugs TableDurgaNadellaNoch keine Bewertungen
- (Hari 8) Risk MatriksDokument1 Seite(Hari 8) Risk MatrikslubangjarumNoch keine Bewertungen
- 1.1 Plumbing History and Terminologies - Building Utilities 1 (Course Materials)Dokument13 Seiten1.1 Plumbing History and Terminologies - Building Utilities 1 (Course Materials)Princessdy CocadizNoch keine Bewertungen
- MZ 14Dokument68 SeitenMZ 14Robert AndrejašNoch keine Bewertungen
- Tropocells 4 Pages PDF Format January 2011Dokument4 SeitenTropocells 4 Pages PDF Format January 2011robertoblumandradeNoch keine Bewertungen
- Radiology X-Rayfilm ScreensDokument39 SeitenRadiology X-Rayfilm ScreensFourthMolar.comNoch keine Bewertungen
- Autocoid PharmacologyDokument29 SeitenAutocoid PharmacologyLyadelou Fortu100% (1)
- Wastewater Treatment Plant Operator I (WWTPOI)Dokument2 SeitenWastewater Treatment Plant Operator I (WWTPOI)Rahmi ArslanNoch keine Bewertungen
- CPD Questions For Volume 21 Issue 3Dokument4 SeitenCPD Questions For Volume 21 Issue 3KeeranmayeeishraNoch keine Bewertungen
- What Is Medical DeontologyDokument11 SeitenWhat Is Medical DeontologyExorticNoch keine Bewertungen
- Experiential Techniques and Therapeutic Relationship in The Treatment of Narcissistic Personality Disorder: The Case of LauraDokument14 SeitenExperiential Techniques and Therapeutic Relationship in The Treatment of Narcissistic Personality Disorder: The Case of Lauraconsulta.nicolaslabbeNoch keine Bewertungen
- Acute Calculous Cholecystitis Strasberg 2008 NEJMDokument8 SeitenAcute Calculous Cholecystitis Strasberg 2008 NEJMFrancisco Castro100% (1)
- Tesis vITAMIN C CONTENT IN FRUITSDokument24 SeitenTesis vITAMIN C CONTENT IN FRUITSHema JothyNoch keine Bewertungen
- Intracanal Medicaments and IrrigantsDokument85 SeitenIntracanal Medicaments and IrrigantsAmit Abbey100% (1)
- Beneficial Effects of Ozone Therapy On Oxidative Stress, Cardiac Functions and Clinical Findings in Patients With Heart Failure Reduced Ejection FractionDokument8 SeitenBeneficial Effects of Ozone Therapy On Oxidative Stress, Cardiac Functions and Clinical Findings in Patients With Heart Failure Reduced Ejection FractionCarlosAlbertoCoutinhoNoch keine Bewertungen
- Living With Feral Cats in YumaDokument2 SeitenLiving With Feral Cats in YumaHumane Society of YumaNoch keine Bewertungen
- Nikolas Rose - Disorders Witouht BordersDokument21 SeitenNikolas Rose - Disorders Witouht BordersPelículasVeladasNoch keine Bewertungen
- Stable Bleaching PowderDokument1 SeiteStable Bleaching PowderAbhishek SharmaNoch keine Bewertungen
- (Trabajo) LRAMP - Linehan PDFDokument7 Seiten(Trabajo) LRAMP - Linehan PDFBreno PMNoch keine Bewertungen
- MedsDokument2 SeitenMedsRuel MaddawinNoch keine Bewertungen
- Medical Terminology SyllabusDokument3 SeitenMedical Terminology SyllabusSalman AfrozeNoch keine Bewertungen
- Psicoterapia Interpersonal en El Tratamiento de La Depresión MayorDokument11 SeitenPsicoterapia Interpersonal en El Tratamiento de La Depresión MayorAndrea MiñoNoch keine Bewertungen
- Tutorial Assignment Week 14 With AnswerDokument4 SeitenTutorial Assignment Week 14 With AnswerCik Wynn100% (1)
- CAM101 Complete Course Notes Reduced SizeDokument174 SeitenCAM101 Complete Course Notes Reduced SizehaydenfarquharNoch keine Bewertungen
- ResumeDokument4 SeitenResumeapi-283952616Noch keine Bewertungen
- Dan CV WordDokument4 SeitenDan CV WorddsnavarretteNoch keine Bewertungen
- Diagnosis & Management of NstemiDokument26 SeitenDiagnosis & Management of NstemiwlshakespeareNoch keine Bewertungen
- Annex"B": Subject: Application For Voluntary Confinement For Treatment and RehabilitationDokument3 SeitenAnnex"B": Subject: Application For Voluntary Confinement For Treatment and RehabilitationShaila GonzalesNoch keine Bewertungen
- Supporting Significant Life EventsDokument5 SeitenSupporting Significant Life Eventschandni0810100% (1)