Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Product Recommendation Hyster Forklift Trucks, Electric J1.60XMTDokument1 SeiteProduct Recommendation Hyster Forklift Trucks, Electric J1.60XMTNelson ConselhoNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- 40 RT-flex Control-System Rev01Dokument68 Seiten40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- PEDokument12 SeitenPEMae Ann Base RicafortNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Chapter Three: 1 - The Coarse Grain SoilsDokument21 SeitenChapter Three: 1 - The Coarse Grain SoilsSalih MohayaddinNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Mini Project 1 - 1Dokument9 SeitenMini Project 1 - 1Sameer BaraNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Smoldering Combustion: Guillermo ReinDokument20 SeitenSmoldering Combustion: Guillermo ReinAhmed HussainNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Electrical Power System Device Function NumberDokument2 SeitenElectrical Power System Device Function Numberdan_teegardenNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Procter and Gamble-1Dokument5 SeitenProcter and Gamble-1Abegiel MendozaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Table 1 Minimum Separation DistancesDokument123 SeitenTable 1 Minimum Separation DistancesjhonNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Me8072 Renewable Sources of EnergyDokument13 SeitenMe8072 Renewable Sources of EnergyNallappan Rajj ANoch keine Bewertungen
- Class 12 - Maths - MatricesDokument87 SeitenClass 12 - Maths - MatricesAishwarya MishraNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Present Simple TaskDokument3 SeitenPresent Simple TaskMaria AlejandraNoch keine Bewertungen
- Navy Supplement To The DOD Dictionary of Military and Associated Terms, 2011Dokument405 SeitenNavy Supplement To The DOD Dictionary of Military and Associated Terms, 2011bateljupko100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- AR BuildingDokument819 SeitenAR BuildingShithin KrishnanNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Pre RmoDokument4 SeitenPre RmoSangeeta Mishra100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Dialog Bahasa InggirsDokument2 SeitenDialog Bahasa InggirsKeRtha NeghaRaNoch keine Bewertungen
- Aircraft Design Course PhillStocking 4.2Dokument48 SeitenAircraft Design Course PhillStocking 4.2ugurugur1982Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Monkeys PawDokument4 SeitenMonkeys PawKaitlin HartmanNoch keine Bewertungen
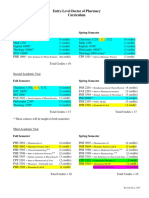
- Pharmd CurriculumDokument18 SeitenPharmd Curriculum5377773Noch keine Bewertungen
- UC Lennox Serie 13 Acx Merit R-410aDokument52 SeitenUC Lennox Serie 13 Acx Merit R-410ajmurcia80Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Pref - 2 - Grammar 1.2 - Revisión Del IntentoDokument2 SeitenPref - 2 - Grammar 1.2 - Revisión Del IntentoJuan M. Suarez ArevaloNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Convection Concentric Annulus Vertical Cylinders Filling Porous MediaDokument17 SeitenConvection Concentric Annulus Vertical Cylinders Filling Porous MediakarthikeyanNoch keine Bewertungen
- Relationsh Between EM and Young S ModuliDokument7 SeitenRelationsh Between EM and Young S ModuliDwight AndersonNoch keine Bewertungen
- Southwest Airlines Final ReportDokument16 SeitenSouthwest Airlines Final Reportapi-427311067Noch keine Bewertungen
- Exercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresDokument14 SeitenExercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresHasmaye PintoNoch keine Bewertungen
- The Wilson Quarterly: The World's New Numbers by Martin WalkerDokument13 SeitenThe Wilson Quarterly: The World's New Numbers by Martin WalkerDavid WeekNoch keine Bewertungen
- Frontinus - Water Management of RomeDokument68 SeitenFrontinus - Water Management of RomezElfmanNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Eliminating Oscillation Between Parallel MnosfetsDokument6 SeitenEliminating Oscillation Between Parallel MnosfetsCiprian BirisNoch keine Bewertungen
- Vallarpadam Terminal ChallengesDokument3 SeitenVallarpadam Terminal Challengespriya rajeev100% (1)
- Banachek UnlimitedDokument34 SeitenBanachek UnlimitedserenaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)