Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Box Culvert 2X2Dokument6 SeitenBox Culvert 2X2abhishek singhNoch keine Bewertungen
- Barangay Profile LangkaanDokument47 SeitenBarangay Profile LangkaanIbn Batuta50% (2)
- Automation and Troubleshooting of Citrix Group Policy For XenApp & XenDesktop 7.x - ArchitectureDokument57 SeitenAutomation and Troubleshooting of Citrix Group Policy For XenApp & XenDesktop 7.x - ArchitectureGowtam DharmarajNoch keine Bewertungen
- User Manual Cuplok (10-2006)Dokument51 SeitenUser Manual Cuplok (10-2006)humaidjafri60% (5)
- FM Fire Pump Inspection Checklist and FormDokument4 SeitenFM Fire Pump Inspection Checklist and Formkrunalb@inNoch keine Bewertungen
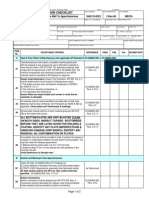
- SAIC-D-2023 Rev 2Dokument2 SeitenSAIC-D-2023 Rev 2ரமேஷ் பாலக்காடுNoch keine Bewertungen
- O Socrealizmu (Jugoslovenski Spomenici)Dokument5 SeitenO Socrealizmu (Jugoslovenski Spomenici)Re Born100% (2)
- Green Building News ClippingsDokument15 SeitenGreen Building News ClippingsIbn BatutaNoch keine Bewertungen
- CLM WRKSHP 03v05Dokument66 SeitenCLM WRKSHP 03v05Ibn BatutaNoch keine Bewertungen
- Post Construction Evaluation Survey GuideDokument4 SeitenPost Construction Evaluation Survey GuideIbn BatutaNoch keine Bewertungen
- NDCC Rapid Assessment Format & Notes 28-May-08Dokument17 SeitenNDCC Rapid Assessment Format & Notes 28-May-08Ibn BatutaNoch keine Bewertungen
- NOTESDokument1 SeiteNOTESIbn BatutaNoch keine Bewertungen
- NC II CarpentryDokument66 SeitenNC II CarpentryIbn BatutaNoch keine Bewertungen
- RP 2.1a Interior Design and Space PlanningDokument3 SeitenRP 2.1a Interior Design and Space PlanningIbn BatutaNoch keine Bewertungen
- Art MovementsDokument2 SeitenArt MovementsIbn BatutaNoch keine Bewertungen
- Principles DesignDokument1 SeitePrinciples Designapi-279889431Noch keine Bewertungen
- Strong Points and Weak PointsDokument2 SeitenStrong Points and Weak PointsIbn BatutaNoch keine Bewertungen
- Chapter I and 3 - Research MethodDokument9 SeitenChapter I and 3 - Research MethodIbn BatutaNoch keine Bewertungen
- Chapter I and 3 - Research MethodDokument9 SeitenChapter I and 3 - Research MethodIbn BatutaNoch keine Bewertungen
- Research Format 3-12-12Dokument6 SeitenResearch Format 3-12-12Gilbert JavierNoch keine Bewertungen
- Faq PoiDokument9 SeitenFaq PoiKishan BhowmikNoch keine Bewertungen
- Building Energy Performance Simulation Tools - A Life-Cycle and Interoperable PerspectiveDokument49 SeitenBuilding Energy Performance Simulation Tools - A Life-Cycle and Interoperable Perspectivehb_scribNoch keine Bewertungen
- Get Started With DropboxDokument10 SeitenGet Started With DropboxYan HakimNoch keine Bewertungen
- Beyond RISC - The Post-RISC Architecture Submitted To: IEEE Micro 3/96Dokument20 SeitenBeyond RISC - The Post-RISC Architecture Submitted To: IEEE Micro 3/96Andreas DelisNoch keine Bewertungen
- 8254 - Programmable Interval TimerDokument17 Seiten8254 - Programmable Interval TimerPraveen Kumar ReddyNoch keine Bewertungen
- AKROUSH, Et Al. (2016) - CFRP Shear Strengthening of Reinforced Concrete Beams in Zones of Combined Shear and Normal StressesDokument18 SeitenAKROUSH, Et Al. (2016) - CFRP Shear Strengthening of Reinforced Concrete Beams in Zones of Combined Shear and Normal StressesDaniel GuedesNoch keine Bewertungen
- Sika Fibre Selection ChartDokument2 SeitenSika Fibre Selection ChartjeffNoch keine Bewertungen
- MML Commands: Object InstructionDokument3 SeitenMML Commands: Object Instructionelectronique12Noch keine Bewertungen
- Juno Lighting Price Book Trac-Master Distributor 6-76Dokument4 SeitenJuno Lighting Price Book Trac-Master Distributor 6-76Alan MastersNoch keine Bewertungen
- Is 2116 1980Dokument13 SeitenIs 2116 1980namdev bkNoch keine Bewertungen
- The Unfolding Stories OF Vitthal (Ghui) Temple Mahal, NagpurDokument11 SeitenThe Unfolding Stories OF Vitthal (Ghui) Temple Mahal, Nagpursecretary ideas alumni associationNoch keine Bewertungen
- Confronting The Errors and Omissions Taboo Up FrontDokument3 SeitenConfronting The Errors and Omissions Taboo Up FrontabobeedoNoch keine Bewertungen
- Girishpote DBA KUWAITDokument7 SeitenGirishpote DBA KUWAITMusa TahirliNoch keine Bewertungen
- NotepadDokument4 SeitenNotepadprithrajNoch keine Bewertungen
- Distributed System AssingmentDokument8 SeitenDistributed System AssingmentLoveday OsiagorNoch keine Bewertungen
- MyquoteDokument11 SeitenMyquotehitesh singhNoch keine Bewertungen
- Concrete Beam Design Based On ACI 318-05: D D E A D BDokument3 SeitenConcrete Beam Design Based On ACI 318-05: D D E A D Bisrar hussainNoch keine Bewertungen
- Solar Street LightDokument3 SeitenSolar Street LightGanesh KaleNoch keine Bewertungen
- 4P - 1450 X 1450 - TSPD - Adjacent OpeningDokument1 Seite4P - 1450 X 1450 - TSPD - Adjacent OpeningNagarajan SNoch keine Bewertungen
- D 1501 Service Manual: DevelopDokument229 SeitenD 1501 Service Manual: DevelopJoel RodriguesNoch keine Bewertungen
- 2n Helios Ip User Manual Pb1510 v1.11.0.17Dokument119 Seiten2n Helios Ip User Manual Pb1510 v1.11.0.17jackaugustNoch keine Bewertungen
- Pengaruh Suspender Tipe Vertical Dan Inclined Terhadap Kestabilan Jembatan GantungDokument10 SeitenPengaruh Suspender Tipe Vertical Dan Inclined Terhadap Kestabilan Jembatan GantungMuhammad RidhaNoch keine Bewertungen
- Fan Heater Inverter Laser Clean LC-52 EN GR INSTRUCTIONS MANUALDokument32 SeitenFan Heater Inverter Laser Clean LC-52 EN GR INSTRUCTIONS MANUALmanosmatNoch keine Bewertungen
- Fontana Dam Spillway and Crack Investigation: Mamorrison0@tva - Gov Jarossillon@tva - GovDokument20 SeitenFontana Dam Spillway and Crack Investigation: Mamorrison0@tva - Gov Jarossillon@tva - GovMarcelo ProtzNoch keine Bewertungen