Das könnte Ihnen auch gefallen
- Bowen Family SystemsDokument7 SeitenBowen Family Systemspwhite78100% (1)
- Bowen Family TheoryDokument320 SeitenBowen Family Theorytonifieraru100% (14)
- Transgenerational and Structural Family TherapyDokument19 SeitenTransgenerational and Structural Family Therapynorociel8132100% (3)
- Bowen Family Systems Theory and Practice Illustration and CritiqueDokument15 SeitenBowen Family Systems Theory and Practice Illustration and CritiqueAdriana Ibanescu100% (3)
- Bowenian Family Therapy: Thinking About This ApproachDokument26 SeitenBowenian Family Therapy: Thinking About This ApproachtodorutzaNoch keine Bewertungen
- An Intergenerational Approach to Family TherapyDokument31 SeitenAn Intergenerational Approach to Family TherapyBeatriz Eugenia Guerra100% (5)
- Bowen Eight InterlockingDokument3 SeitenBowen Eight InterlockingVito Achumi Inakha100% (1)
- Murray Bowen's Family Systems TheoryDokument10 SeitenMurray Bowen's Family Systems Theorynorociel8132Noch keine Bewertungen
- Bowen Systems Theory and Mediation TheoryDokument19 SeitenBowen Systems Theory and Mediation TheoryLiliana Butariu100% (1)
- The Bowen Family Theory and Its UsesDokument404 SeitenThe Bowen Family Theory and Its UsesGavroDjurickovic100% (2)
- Couple Conflict and Family SystemsDokument121 SeitenCouple Conflict and Family Systemsmcris101100% (2)
- Family TherapyDokument10 SeitenFamily TherapyKaren Jae Grant CabrillosNoch keine Bewertungen
- Michael E. Kerr - Murray Bowen - Family Evaluation-W. W. Norton Company (1988)Dokument415 SeitenMichael E. Kerr - Murray Bowen - Family Evaluation-W. W. Norton Company (1988)Martis Jonas100% (12)
- A Family Therapy NarrativeDokument14 SeitenA Family Therapy NarrativeEmma SánchezNoch keine Bewertungen
- Couples in Conflict: A Family Systems Approach To Marriage CounselingVon EverandCouples in Conflict: A Family Systems Approach To Marriage CounselingNoch keine Bewertungen
- Counseling Theories Integration Paper Analyzes Bowen's Family Systems TheoryDokument14 SeitenCounseling Theories Integration Paper Analyzes Bowen's Family Systems TheoryErin P. O'Connor100% (3)
- Bowen TheoryDokument6 SeitenBowen TheoryTubocurare100% (2)
- Triangles - Bowen Family Systems - Titelman, PeterDokument436 SeitenTriangles - Bowen Family Systems - Titelman, PeterAna Patricia Mendoza Espinosa100% (8)
- Structural Family TherapyDokument14 SeitenStructural Family TherapyFlorica PodariuNoch keine Bewertungen
- The 8 Concepts of M BDokument70 SeitenThe 8 Concepts of M Beduardobar2000100% (4)
- Colapinto Structural Family TherapyDokument27 SeitenColapinto Structural Family TherapyEmilia Morosan100% (1)
- Systemic Therapy and The Influence of Postmodernism 2000Dokument8 SeitenSystemic Therapy and The Influence of Postmodernism 2000macmat1Noch keine Bewertungen
- Bowen TheoryDokument11 SeitenBowen TheoryJorge MurilloNoch keine Bewertungen
- Systemic Family TherapyDokument19 SeitenSystemic Family TherapyDiego Rojas TorricoNoch keine Bewertungen
- Emotionally Focused Couple Therapy: Addressing Attachment NeedsDokument41 SeitenEmotionally Focused Couple Therapy: Addressing Attachment Needsvaradh24100% (1)
- McGoldrick Et Al 2010 Ch1Dokument20 SeitenMcGoldrick Et Al 2010 Ch1Kells Mar100% (3)
- Demetrios Peratsakis, LPC, ACS and Natalia Tague, LPCDokument21 SeitenDemetrios Peratsakis, LPC, ACS and Natalia Tague, LPCAMY WONG100% (1)
- Genograms - ReferenceDokument21 SeitenGenograms - ReferenceJustin Paul100% (4)
- Working at Relational Depth in Counselling and Psychotherapy - Dave MearnsDokument5 SeitenWorking at Relational Depth in Counselling and Psychotherapy - Dave Mearnsjyjamewy33% (3)
- Techniques in Family TherapyDokument23 SeitenTechniques in Family TherapyAntónio Martins100% (4)
- Greg Madison Existential Palapable 2014Dokument9 SeitenGreg Madison Existential Palapable 2014Natalia O'Connor KornychkovaNoch keine Bewertungen
- Working With Emotion: in Psychodynamic, Cognitive Behavior, and Emotion-Focused PsychotherapyDokument204 SeitenWorking With Emotion: in Psychodynamic, Cognitive Behavior, and Emotion-Focused Psychotherapyirina100% (3)
- Collaborative TherapyDokument9 SeitenCollaborative Therapyisiplaya2013Noch keine Bewertungen
- Circular Questioning As A Therapeutic ToDokument13 SeitenCircular Questioning As A Therapeutic ToNicole Prat CoghlanNoch keine Bewertungen
- Change Process Research in PsychotherapyDokument19 SeitenChange Process Research in PsychotherapyJuanaNoch keine Bewertungen
- Family Therapy: Tupas and TajalaDokument18 SeitenFamily Therapy: Tupas and TajalaEdel CarlosNoch keine Bewertungen
- Bowenian Family TherapyDokument7 SeitenBowenian Family TherapyCybill BlakeNoch keine Bewertungen
- Greenberg - Emotion Focused Therapy (Comunicação) PDFDokument18 SeitenGreenberg - Emotion Focused Therapy (Comunicação) PDFTiago A. G. FonsecaNoch keine Bewertungen
- (Leslie - S. - Greenberg, - Jeanne - C. - Watson) - Emotion-Focused Therapy PDFDokument350 Seiten(Leslie - S. - Greenberg, - Jeanne - C. - Watson) - Emotion-Focused Therapy PDFAllen Wheeler83% (6)
- (Snyder Et Al, 2012) - Integrative Approaches To Couple Therapy PDFDokument12 Seiten(Snyder Et Al, 2012) - Integrative Approaches To Couple Therapy PDFEileen GarcíaNoch keine Bewertungen
- Family Counseling Structural ModelDokument28 SeitenFamily Counseling Structural ModelMuhd Hafeez100% (1)
- Knudson Martin Et Al-2015-Journal of Marital and Family TherapyDokument16 SeitenKnudson Martin Et Al-2015-Journal of Marital and Family TherapyDann Js100% (1)
- Comparing REBT and Person-Centered Counseling TheoriesDokument30 SeitenComparing REBT and Person-Centered Counseling TheoriesIra Affandee100% (1)
- Milan Systemic Family Therapy A Review of 10 EmpiricalDokument26 SeitenMilan Systemic Family Therapy A Review of 10 EmpiricalIramil KaramazovNoch keine Bewertungen
- Differentiation and Power in Couples TherapyDokument183 SeitenDifferentiation and Power in Couples TherapyAndrooschka LeeNoch keine Bewertungen
- Howe, D. (2011) - Attachment Across The Lifecourse: A Brief Introduction. New York: Palgrave MacmillanDokument4 SeitenHowe, D. (2011) - Attachment Across The Lifecourse: A Brief Introduction. New York: Palgrave MacmillanLaura Pearl Kaya100% (1)
- Attachment Narrative PDFDokument12 SeitenAttachment Narrative PDFτασοσ100% (1)
- Emotion-Focused Therapy: A Summary and Overview DR Leslie GreenbergDokument26 SeitenEmotion-Focused Therapy: A Summary and Overview DR Leslie GreenbergRichiNoch keine Bewertungen
- Circular Questioining An Introductory-Guide-Jac Brown PDFDokument6 SeitenCircular Questioining An Introductory-Guide-Jac Brown PDFNelson GalvisNoch keine Bewertungen
- Emotion-Focused Couples’ Communication Program: An Innovative Approach Towards Enhancing Couples’ Communication and Improving Marital SatisfactionVon EverandEmotion-Focused Couples’ Communication Program: An Innovative Approach Towards Enhancing Couples’ Communication and Improving Marital SatisfactionNoch keine Bewertungen
- Structural Family TherapyDokument14 SeitenStructural Family TherapySalmi Sabri100% (1)
- Patterson Cognitive Behavioral Systems ApproachDokument14 SeitenPatterson Cognitive Behavioral Systems ApproachSusana FossaNoch keine Bewertungen
- Integrative Approaches To Supervision PDFDokument219 SeitenIntegrative Approaches To Supervision PDFpentele100% (1)
- Bowen, Minuchin, SatirDokument5 SeitenBowen, Minuchin, SatirSarahNoch keine Bewertungen
- Emotionally Focused Therapy (Eft) and Emotionally Focused Family Therapy (Efft) : A Challenge/opportunity For Systemic and Post-Systemic TherapistsDokument5 SeitenEmotionally Focused Therapy (Eft) and Emotionally Focused Family Therapy (Efft) : A Challenge/opportunity For Systemic and Post-Systemic TherapistsEFTcouplesNoch keine Bewertungen
- Emotion in Psychotherapy A Practice Friendly ReviewDokument20 SeitenEmotion in Psychotherapy A Practice Friendly ReviewpsicandreiaNoch keine Bewertungen
- Murray Bowen's Insights Into Family DynamicsDokument21 SeitenMurray Bowen's Insights Into Family DynamicsLea Tan100% (2)
- Survival InjunctionsDokument12 SeitenSurvival InjunctionsRobinNoch keine Bewertungen
- Systems Theory and Family Therapy: A PrimerVon EverandSystems Theory and Family Therapy: A PrimerBewertung: 5 von 5 Sternen5/5 (1)
- Bowen family systems theory in Christian ministry: Grappling with Theory and its Application Through a Biblical LensVon EverandBowen family systems theory in Christian ministry: Grappling with Theory and its Application Through a Biblical LensBewertung: 5 von 5 Sternen5/5 (1)
- Adult Attachment InterviewDokument11 SeitenAdult Attachment InterviewAndreea Serpisor100% (1)
- Schema Therapy For Personality Disorders A Qualitative Study of Patients and Therapists Perspectives PDFDokument16 SeitenSchema Therapy For Personality Disorders A Qualitative Study of Patients and Therapists Perspectives PDFMari ForgachNoch keine Bewertungen
- Schema Therapy For Personality Disorders A Qualitative Study of Patients and Therapists Perspectives PDFDokument16 SeitenSchema Therapy For Personality Disorders A Qualitative Study of Patients and Therapists Perspectives PDFMari ForgachNoch keine Bewertungen
- SensateFocus M&J 2014 PDFDokument13 SeitenSensateFocus M&J 2014 PDFMari Forgach100% (1)
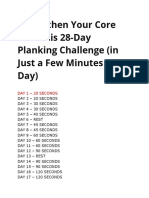
- 28-Day Planking Challenge Strengthen Your Core in MinutesDokument2 Seiten28-Day Planking Challenge Strengthen Your Core in MinutesMari ForgachNoch keine Bewertungen
- Clarifying Sensate Focus and Sex as a Natural FunctionDokument13 SeitenClarifying Sensate Focus and Sex as a Natural FunctionMari Forgach100% (1)
- Individual Family ConstellationsDokument11 SeitenIndividual Family ConstellationsMadalina-Irina Tanaselea100% (5)
- 28-Day Planking Challenge Strengthen Your Core in MinutesDokument2 Seiten28-Day Planking Challenge Strengthen Your Core in MinutesMari ForgachNoch keine Bewertungen
- 28-Day Planking Challenge Strengthen Your Core in MinutesDokument2 Seiten28-Day Planking Challenge Strengthen Your Core in MinutesMari ForgachNoch keine Bewertungen
- Strengthen Your Core With This 28Dokument2 SeitenStrengthen Your Core With This 28Mari ForgachNoch keine Bewertungen
- Transcripts of Carl Rogers' Therapy SessionsDokument109 SeitenTranscripts of Carl Rogers' Therapy SessionsMari Forgach100% (3)
- Robert Waldinger & Alan M. Jacobson: The Initial Psychiatric InterviewDokument4 SeitenRobert Waldinger & Alan M. Jacobson: The Initial Psychiatric InterviewMari Forgach100% (1)
- Manual Controlador C90Dokument442 SeitenManual Controlador C90Fabián MejíaNoch keine Bewertungen
- Arduino The Ultimate Beginners Guide To Arduino Learn How To Get Started With Arduino Programming Projects and More PDFDokument33 SeitenArduino The Ultimate Beginners Guide To Arduino Learn How To Get Started With Arduino Programming Projects and More PDFefrain100% (1)
- Rohtak:: ICT Hub For E-Governance in HaryanaDokument2 SeitenRohtak:: ICT Hub For E-Governance in HaryanaAr Aayush GoelNoch keine Bewertungen
- Study of the Courier Industry at BookMyPacketDokument34 SeitenStudy of the Courier Industry at BookMyPacketPiyush MittalNoch keine Bewertungen
- (JPP-1) - (Indefinite Integration) - 11th SepDokument52 Seiten(JPP-1) - (Indefinite Integration) - 11th Sepfunnyvideos. comNoch keine Bewertungen
- Physical Properties of SolutionsDokument23 SeitenPhysical Properties of Solutions董青天Noch keine Bewertungen
- Sri Chaitanya IIT Academy., India.: PhysicsDokument12 SeitenSri Chaitanya IIT Academy., India.: PhysicsSridhar ReddyNoch keine Bewertungen
- Netiquette & Class RulesDokument1 SeiteNetiquette & Class RulesDanny LabordoNoch keine Bewertungen
- Introduction To Voice AlarmDokument58 SeitenIntroduction To Voice AlarmShaaban HassanNoch keine Bewertungen
- Muhammad Usama: Internship at Ibrahim Fibres Limited, Polyester PlantDokument20 SeitenMuhammad Usama: Internship at Ibrahim Fibres Limited, Polyester PlantUsamaNoch keine Bewertungen
- Ebook Childhood and Adolescence Voyages in Development 6Th Edition Rathus Test Bank Full Chapter PDFDokument64 SeitenEbook Childhood and Adolescence Voyages in Development 6Th Edition Rathus Test Bank Full Chapter PDFolwennathan731y100% (8)
- SH BSC Hons Pre Registration Nursing PDFDokument104 SeitenSH BSC Hons Pre Registration Nursing PDFJogendra Singh PatelNoch keine Bewertungen
- Subscriber Loop Design LectureDokument36 SeitenSubscriber Loop Design LectureAlas Mallari DonatoNoch keine Bewertungen
- PBL62 1 30M3Dokument1 SeitePBL62 1 30M3Hai Tran HongNoch keine Bewertungen
- Chapter 1 PPT (Compressibility and Consolidation)Dokument65 SeitenChapter 1 PPT (Compressibility and Consolidation)Eba GetachewNoch keine Bewertungen
- Analysis, Design and Implementation of Zero-Current-Switching Resonant Converter DC-DC Buck ConverterDokument12 SeitenAnalysis, Design and Implementation of Zero-Current-Switching Resonant Converter DC-DC Buck Converterdaber_huny20Noch keine Bewertungen
- What Is Change Management and Why Is It Important (Discussion Board)Dokument2 SeitenWhat Is Change Management and Why Is It Important (Discussion Board)Arun KumarNoch keine Bewertungen
- 1-2 SemestrDokument83 Seiten1-2 SemestrАнтон СелезневNoch keine Bewertungen
- Ipc2012 90095Dokument11 SeitenIpc2012 90095Marcelo Varejão CasarinNoch keine Bewertungen
- 2 X 660MWNCC POWER PROJECT UPS SIZING CALCULATIONDokument5 Seiten2 X 660MWNCC POWER PROJECT UPS SIZING CALCULATIONkkumar_717405Noch keine Bewertungen
- Design of Hydroelectric Power PlantsDokument6 SeitenDesign of Hydroelectric Power PlantsPDN PRGNoch keine Bewertungen
- TTLA0649-Monitor ZX-3Dokument23 SeitenTTLA0649-Monitor ZX-3saufanNoch keine Bewertungen
- Electronic Devices and Circuit TheoryDokument32 SeitenElectronic Devices and Circuit TheoryIñaki Zuriel ConstantinoNoch keine Bewertungen
- Comparison of fibre migration in different yarn bodiesDokument5 SeitenComparison of fibre migration in different yarn bodiesJerin JosephNoch keine Bewertungen
- G5 - CLC 30Dokument5 SeitenG5 - CLC 30Phuong AnhNoch keine Bewertungen
- CA2005 User Manual 1.3-Custom-FDokument34 SeitenCA2005 User Manual 1.3-Custom-FDinesh SreedharanNoch keine Bewertungen
- Computers & Industrial Engineering: Guohui Zhang, Xinyu Shao, Peigen Li, Liang GaoDokument10 SeitenComputers & Industrial Engineering: Guohui Zhang, Xinyu Shao, Peigen Li, Liang Gaocloud69windNoch keine Bewertungen
- Lattice SeminarDokument48 SeitenLattice SeminarNaina JabbarNoch keine Bewertungen
- Altair's Student Guides - CAE and Design Optimization - AdvancedDokument70 SeitenAltair's Student Guides - CAE and Design Optimization - AdvancedKFourMetrics100% (11)
- Cambridge International Examinations: Additional Mathematics 4037/12 May/June 2017Dokument11 SeitenCambridge International Examinations: Additional Mathematics 4037/12 May/June 2017Ms jennyNoch keine Bewertungen