Das könnte Ihnen auch gefallen
- Occupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyDokument12 SeitenOccupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyIlvita MayasariNoch keine Bewertungen
- A Telehealth Approach To Oropharyngeal Dysphagia TherapyDokument5 SeitenA Telehealth Approach To Oropharyngeal Dysphagia TherapyHeriberto Aguirre MenesesNoch keine Bewertungen
- Example of PHD Research ProposalDokument2 SeitenExample of PHD Research ProposalMuhammad Khurram ShahzadNoch keine Bewertungen
- Telehealth in Audiology: An Integrative ReviewDokument8 SeitenTelehealth in Audiology: An Integrative ReviewRUBÉN TOMÁS CRUZNoch keine Bewertungen
- Content ServerDokument14 SeitenContent ServerDilfera HermiatiNoch keine Bewertungen
- Prelim Exam Block 2 Group 3Dokument5 SeitenPrelim Exam Block 2 Group 3Sufina AnnNoch keine Bewertungen
- Metaanalisis Castro Et Al. 2019Dokument37 SeitenMetaanalisis Castro Et Al. 2019LauraNoch keine Bewertungen
- Bommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Dokument14 SeitenBommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Maximiliano AzconaNoch keine Bewertungen
- Martino, D. (2023) - Treatment Failure in Persisten Tic Disorders...Dokument15 SeitenMartino, D. (2023) - Treatment Failure in Persisten Tic Disorders...cuautzinNoch keine Bewertungen
- Evaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersDokument10 SeitenEvaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersAbu Faris Al-MandariNoch keine Bewertungen
- BMC Pediatrics: Effectiveness of Physical Therapy Interventions For Children With Cerebral Palsy: A Systematic ReviewDokument10 SeitenBMC Pediatrics: Effectiveness of Physical Therapy Interventions For Children With Cerebral Palsy: A Systematic ReviewERICKNoch keine Bewertungen
- Yjmt 30 1992090Dokument13 SeitenYjmt 30 1992090Luis Sebastian Arango OspinaNoch keine Bewertungen
- A Treatment Schedule of Conventional Physical Therapy Provided To Enhance Upper Limb Sensorimotor Recovery After Stroke Expert Criterion Validity and Intra-Rater ReliabilityDokument10 SeitenA Treatment Schedule of Conventional Physical Therapy Provided To Enhance Upper Limb Sensorimotor Recovery After Stroke Expert Criterion Validity and Intra-Rater ReliabilityGeraldo MoraesNoch keine Bewertungen
- Impact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForDokument38 SeitenImpact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForImpact JournalsNoch keine Bewertungen
- Disfagia OFDokument13 SeitenDisfagia OFSebastián Contreras CubillosNoch keine Bewertungen
- Telehealth RirinDokument12 SeitenTelehealth RirinririnsityalfiahNoch keine Bewertungen
- Effects of Internet-Based Psycho-Educational Interventions On Mental Health and Quality of Life Among Cancer PatientsDokument12 SeitenEffects of Internet-Based Psycho-Educational Interventions On Mental Health and Quality of Life Among Cancer PatientsflorgilNoch keine Bewertungen
- NGC 8208Dokument12 SeitenNGC 8208Alvaro Carlos Calvo ValenciaNoch keine Bewertungen
- Investigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice ExperimentDokument13 SeitenInvestigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice Experimenttherese BNoch keine Bewertungen
- Health Care Professionals' Experiences and Perspectives On Using Telehealth For Home-Based Palliative Care: Protocol For A Scoping ReviewDokument7 SeitenHealth Care Professionals' Experiences and Perspectives On Using Telehealth For Home-Based Palliative Care: Protocol For A Scoping Reviewshaza ameliaNoch keine Bewertungen
- Complementary Therapies in Clinical PracticeDokument18 SeitenComplementary Therapies in Clinical PracticeNgaWa ChowNoch keine Bewertungen
- Homebasedtelehealth PDFDokument6 SeitenHomebasedtelehealth PDFdaniel serraniNoch keine Bewertungen
- Putting Life in Years Pliny Telephone Friendship Groups Research Study Pilot Randomised Controlled TrialDokument12 SeitenPutting Life in Years Pliny Telephone Friendship Groups Research Study Pilot Randomised Controlled TrialMahmoud Abd ElazizNoch keine Bewertungen
- J Telemed Telecare 2011 Steel 109 17Dokument10 SeitenJ Telemed Telecare 2011 Steel 109 17LoguitosNoch keine Bewertungen
- Adherence Interventions and Outcomes of Tuberculosis Treatment in Low - and Middle-Income Countries (Lmic) : A Systematic Review ProtocolDokument6 SeitenAdherence Interventions and Outcomes of Tuberculosis Treatment in Low - and Middle-Income Countries (Lmic) : A Systematic Review Protocolijmb333Noch keine Bewertungen
- Applied Sciences: Post-Tuberculosis (TB) Treatment: The Role of Surgery and RehabilitationDokument18 SeitenApplied Sciences: Post-Tuberculosis (TB) Treatment: The Role of Surgery and Rehabilitationraja yasminNoch keine Bewertungen
- Acceptance and Commitment Therapy in Cancer: Review of Applications and FindingsDokument27 SeitenAcceptance and Commitment Therapy in Cancer: Review of Applications and FindingsJuan Alberto GonzálezNoch keine Bewertungen
- Comparing Digital To Conventional Physical Therapy For ChronicDokument18 SeitenComparing Digital To Conventional Physical Therapy For ChronickiranNoch keine Bewertungen
- Carlozzi-14 RS Outcomes HDDokument20 SeitenCarlozzi-14 RS Outcomes HDMARIA MONTSERRAT SOMOZA MONCADANoch keine Bewertungen
- A Study of Proactive Ethics Consultation For CriticallyDokument18 SeitenA Study of Proactive Ethics Consultation For CriticallyJENIFER KARINA PUTZ LORENZINoch keine Bewertungen
- Lung HN CancerDokument11 SeitenLung HN CancerFlorinaNoch keine Bewertungen
- Intensive & Critical Care Nursing: Ziad Alostaz, Louise Rose, Sangeeta Mehta, Linda Johnston, Craig DaleDokument11 SeitenIntensive & Critical Care Nursing: Ziad Alostaz, Louise Rose, Sangeeta Mehta, Linda Johnston, Craig DalecindyNoch keine Bewertungen
- Oropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysisDokument7 SeitenOropharyngeal and Tongue Exercises (Myofunctional Therapy) For Snoring: A Systematic Review and Meta-AnalysissirahNoch keine Bewertungen
- Journal Homepage: - : Introduction:-Objectives of The StudyDokument4 SeitenJournal Homepage: - : Introduction:-Objectives of The StudyIJAR JOURNALNoch keine Bewertungen
- Telepsiquiatria Meta Analisis 1Dokument11 SeitenTelepsiquiatria Meta Analisis 1daniel serraniNoch keine Bewertungen
- Wong Et Al-2015-Health & Social Care in The CommunityDokument13 SeitenWong Et Al-2015-Health & Social Care in The CommunityJoNoch keine Bewertungen
- HayesCAREER SharedDokument24 SeitenHayesCAREER SharedZhongxing YuNoch keine Bewertungen
- Effectiveness of Telemedicine: A Systematic Review of ReviewsDokument31 SeitenEffectiveness of Telemedicine: A Systematic Review of ReviewsaNoch keine Bewertungen
- NT and Conventional Medicine PDFDokument10 SeitenNT and Conventional Medicine PDFneuralterapianetNoch keine Bewertungen
- Case Study #3Dokument26 SeitenCase Study #3Reshma MohabeirNoch keine Bewertungen
- Artigo Mobilização PrecoceDokument9 SeitenArtigo Mobilização PrecoceLuciana AlexandreNoch keine Bewertungen
- The Pain, Agitation, and Delirium Practice Guidelines For Adult Critically Ill Patients: A Post-Publication PerspectiveDokument9 SeitenThe Pain, Agitation, and Delirium Practice Guidelines For Adult Critically Ill Patients: A Post-Publication Perspectivedebby claudiNoch keine Bewertungen
- 1 s2.0 S1201971214017214 Main PDFDokument5 Seiten1 s2.0 S1201971214017214 Main PDFYohanna ekasntNoch keine Bewertungen
- Severe Head Injury Clinical PathwayDokument7 SeitenSevere Head Injury Clinical PathwaytheodoruskevinNoch keine Bewertungen
- A Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsDokument7 SeitenA Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsInternational Journal of Application or Innovation in Engineering & ManagementNoch keine Bewertungen
- Summary of Purposes and ObjectivesDokument19 SeitenSummary of Purposes and Objectivesrodolfo opido100% (1)
- Effect of TelenursingDokument17 SeitenEffect of Telenursingirma nur amaliaNoch keine Bewertungen
- Nursing 440 - Nursing Leadership and Innovation Paper October 2014Dokument12 SeitenNursing 440 - Nursing Leadership and Innovation Paper October 2014api-242437021Noch keine Bewertungen
- Mobile Health (Mhealth) Versus Clinic-Based Group Intervention For People With Serious Mental Illness: A Randomized Controlled TrialDokument8 SeitenMobile Health (Mhealth) Versus Clinic-Based Group Intervention For People With Serious Mental Illness: A Randomized Controlled TrialOlivia NasarreNoch keine Bewertungen
- A Systematic Review of Telehealth Applications in Audiology: OriginalDokument20 SeitenA Systematic Review of Telehealth Applications in Audiology: Originalaimen_riyadhNoch keine Bewertungen
- Mental Health Services Research Methodology 2002Dokument8 SeitenMental Health Services Research Methodology 2002Kats CoelloNoch keine Bewertungen
- Cost-Effectiveness of Early Intervention in First-Episode Psychosis: Economic Evaluation of A Randomised Controlled Trial (The OPUS Study)Dokument8 SeitenCost-Effectiveness of Early Intervention in First-Episode Psychosis: Economic Evaluation of A Randomised Controlled Trial (The OPUS Study)Carlos A Luna CruzNoch keine Bewertungen
- 2019 Cognitive Rehabilitation For Cancer Related Cognitive DisfunctionDokument27 Seiten2019 Cognitive Rehabilitation For Cancer Related Cognitive DisfunctionAlba Sueiro DominguezNoch keine Bewertungen
- Neurologist Communicationg The Diagnosis of ELADokument9 SeitenNeurologist Communicationg The Diagnosis of ELAHabib G. Moutran BarrosoNoch keine Bewertungen
- Perez Mengual, M. - s0134775 (Verslag)Dokument61 SeitenPerez Mengual, M. - s0134775 (Verslag)Silvio MoralesNoch keine Bewertungen
- Telesalud - FisioterapiaDokument8 SeitenTelesalud - FisioterapiaManuel OlarteNoch keine Bewertungen
- Published Researches in The Year 2010Dokument16 SeitenPublished Researches in The Year 2010hsrimediaNoch keine Bewertungen
- A Survey of Practice Patterns For Rehabilitation Post Elbow FractureDokument11 SeitenA Survey of Practice Patterns For Rehabilitation Post Elbow Fracturejeremy1roseNoch keine Bewertungen
- Truijen2022 Article EffectOfHome-basedVirtualRealiDokument12 SeitenTruijen2022 Article EffectOfHome-basedVirtualRealiSM199021Noch keine Bewertungen
- IV GaugesDokument1 SeiteIV Gaugesjustin_saneNoch keine Bewertungen
- Peptic UlcerrDokument3 SeitenPeptic Ulcerrjustin_saneNoch keine Bewertungen
- Injection Site Cheat Sheet PDFDokument2 SeitenInjection Site Cheat Sheet PDFjustin_sane100% (2)
- Common Drug Stems Cheat SheetDokument2 SeitenCommon Drug Stems Cheat SheetCharis Mae DimaculanganNoch keine Bewertungen
- Improving Postoperative Pain Management What Are.40Dokument6 SeitenImproving Postoperative Pain Management What Are.40Luz Adriana Flores PalafoxNoch keine Bewertungen
- Risk For Infection Pneumonia Nursing Care PlanDokument1 SeiteRisk For Infection Pneumonia Nursing Care Planjustin_sane100% (1)
- Microsoft Word - Pneumonia Education EnglishDokument9 SeitenMicrosoft Word - Pneumonia Education Englishjustin_saneNoch keine Bewertungen
- HemodialysisDokument2 SeitenHemodialysisjustin_saneNoch keine Bewertungen
- DiagnosticDokument5 SeitenDiagnosticjustin_saneNoch keine Bewertungen
- Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationDokument2 SeitenAssessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale Evaluationjustin_saneNoch keine Bewertungen
- 2 Acute Pain Chronic Renal Failure Nursing Care PlansDokument5 Seiten2 Acute Pain Chronic Renal Failure Nursing Care Plansjustin_saneNoch keine Bewertungen
- Hyperthermia Pneumonia Nursing Care PlanDokument1 SeiteHyperthermia Pneumonia Nursing Care Planjustin_saneNoch keine Bewertungen
- DMDokument10 SeitenDMjustin_saneNoch keine Bewertungen
- Physical AssessmentDokument29 SeitenPhysical Assessmentjustin_saneNoch keine Bewertungen
- PneumoniaDokument17 SeitenPneumoniajustin_saneNoch keine Bewertungen
- Ineffective Airway Clearance Pneumonia Nursing Care PlanDokument1 SeiteIneffective Airway Clearance Pneumonia Nursing Care Planjustin_sane100% (4)
- Other Possible Nursing Care PlansDokument1 SeiteOther Possible Nursing Care Plansjustin_saneNoch keine Bewertungen
- 2 Acute Pain Chronic Renal Failure Nursing Care PlansDokument5 Seiten2 Acute Pain Chronic Renal Failure Nursing Care Plansjustin_saneNoch keine Bewertungen
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDokument1 SeiteIneffective Breathing Pattern Pneumonia Nursing Care Planjustin_saneNoch keine Bewertungen
- 5 Altered Nutrition Less Than Body Requirements Chronic Renal Failure Nursing Care PlansDokument3 Seiten5 Altered Nutrition Less Than Body Requirements Chronic Renal Failure Nursing Care Plansjustin_sane40% (5)
- Chilldeck KTV & Music Lounge: Free Five (5) Songs in Every Three (3) Buckets of DrinksDokument1 SeiteChilldeck KTV & Music Lounge: Free Five (5) Songs in Every Three (3) Buckets of Drinksjustin_saneNoch keine Bewertungen
- Risk For Infection Pneumonia Nursing Care PlanDokument1 SeiteRisk For Infection Pneumonia Nursing Care Planjustin_sane100% (1)
- Impaired Gas Exchange Pneumonia Nursing Care PlanDokument1 SeiteImpaired Gas Exchange Pneumonia Nursing Care Planjustin_saneNoch keine Bewertungen
- Air Passenger Bill of RightsDokument12 SeitenAir Passenger Bill of RightsAldan Subion Avila100% (1)
- High-Rise Climb V0.6a Smokeydots PDFDokument10 SeitenHigh-Rise Climb V0.6a Smokeydots PDFHer Lan ONoch keine Bewertungen
- X25Dokument10 SeitenX25RajNoch keine Bewertungen
- Service Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8Dokument8 SeitenService Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8GutsavoNoch keine Bewertungen
- Standard C4C End User GuideDokument259 SeitenStandard C4C End User GuideKanali PaariNoch keine Bewertungen
- Marketing Research ProjectDokument37 SeitenMarketing Research ProjectVijay100% (15)
- AKROLEN® PP ICF 30 AM Black (8344) - Akro-PlasticDokument3 SeitenAKROLEN® PP ICF 30 AM Black (8344) - Akro-PlasticalkhalidibaiderNoch keine Bewertungen
- Exit Exam Plan (New)Dokument2 SeitenExit Exam Plan (New)Eleni Semenhi100% (1)
- Table of Contents - YmodDokument4 SeitenTable of Contents - YmodDr.Prakher SainiNoch keine Bewertungen
- Calio Z: Type Series BookletDokument24 SeitenCalio Z: Type Series BookletDan PopescuNoch keine Bewertungen
- SS 531 2006 Code of Practice For Lighting of Work Places Part 1 PDFDokument13 SeitenSS 531 2006 Code of Practice For Lighting of Work Places Part 1 PDFEdmund YoongNoch keine Bewertungen
- DPS Ibak en PDFDokument9 SeitenDPS Ibak en PDFjsenadNoch keine Bewertungen
- EquisetopsidaDokument4 SeitenEquisetopsidax456456456xNoch keine Bewertungen
- Product Management GemsDokument14 SeitenProduct Management GemsVijendra GopaNoch keine Bewertungen
- 1.2 Server Operating SystemDokument20 Seiten1.2 Server Operating SystemAzhar AhmadNoch keine Bewertungen
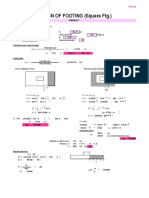
- Design of Footing (Square FTG.) : M Say, L 3.75Dokument2 SeitenDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNoch keine Bewertungen
- A Study of A Skirtless Hovercraft DesignDokument71 SeitenA Study of A Skirtless Hovercraft DesignSunil Kumar P GNoch keine Bewertungen
- Role of SpeakerDokument11 SeitenRole of SpeakerSnehil AnandNoch keine Bewertungen
- Bromate Prove Ulr en 2016-01-06 HintDokument3 SeitenBromate Prove Ulr en 2016-01-06 Hinttata_77Noch keine Bewertungen
- Exercises Service CostingDokument2 SeitenExercises Service Costingashikin dzulNoch keine Bewertungen
- Guide To Downloading and Installing The WebMethods Free Trial Version - Wiki - CommunitiesDokument19 SeitenGuide To Downloading and Installing The WebMethods Free Trial Version - Wiki - CommunitiesHieu NguyenNoch keine Bewertungen
- Reliability EngineerDokument1 SeiteReliability EngineerBesuidenhout Engineering Solutions and ConsultingNoch keine Bewertungen
- Plasticizers For CPE ElastomersDokument8 SeitenPlasticizers For CPE Elastomersbatur42Noch keine Bewertungen
- Vigi Module Selection PDFDokument1 SeiteVigi Module Selection PDFrt1973Noch keine Bewertungen
- Microstrip Antennas: How Do They Work?Dokument2 SeitenMicrostrip Antennas: How Do They Work?Tebogo SekgwamaNoch keine Bewertungen
- Series 90 100cc Pump Parts ManualDokument152 SeitenSeries 90 100cc Pump Parts ManualHernan Garcia67% (3)
- Solution Manual For Labor Relations Development Structure Process 12th Edition Fossum 0077862473 9780077862473Dokument16 SeitenSolution Manual For Labor Relations Development Structure Process 12th Edition Fossum 0077862473 9780077862473savannahzavalaxodtfznisq100% (27)
- Introduction To AccountingDokument36 SeitenIntroduction To AccountingRajnikant PatelNoch keine Bewertungen
- Termsconditions of JionetDokument3 SeitenTermsconditions of JionetskNoch keine Bewertungen
- (English) 362L Stereoselective Wittig Reaction - Synthesis of Ethyl Trans-Cinnamate (#7) (DownSub - Com)Dokument6 Seiten(English) 362L Stereoselective Wittig Reaction - Synthesis of Ethyl Trans-Cinnamate (#7) (DownSub - Com)moNoch keine Bewertungen
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeVon EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeBewertung: 4.5 von 5 Sternen4.5/5 (141)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryVon EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryBewertung: 4.5 von 5 Sternen4.5/5 (157)
- Don't Panic: Taking Control of Anxiety AttacksVon EverandDon't Panic: Taking Control of Anxiety AttacksBewertung: 4 von 5 Sternen4/5 (12)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDVon EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDBewertung: 4.5 von 5 Sternen4.5/5 (167)
- An Autobiography of Trauma: A Healing JourneyVon EverandAn Autobiography of Trauma: A Healing JourneyBewertung: 5 von 5 Sternen5/5 (2)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveVon EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveBewertung: 4 von 5 Sternen4/5 (250)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeVon EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeBewertung: 4.5 von 5 Sternen4.5/5 (49)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackVon EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackBewertung: 4.5 von 5 Sternen4.5/5 (153)
- Breaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingVon EverandBreaking the Chains of Transgenerational Trauma: My Journey from Surviving to ThrivingBewertung: 4.5 von 5 Sternen4.5/5 (30)
- Feeling Great: The Revolutionary New Treatment for Depression and AnxietyVon EverandFeeling Great: The Revolutionary New Treatment for Depression and AnxietyNoch keine Bewertungen
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisVon EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisBewertung: 5 von 5 Sternen5/5 (5)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItVon EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItBewertung: 4.5 von 5 Sternen4.5/5 (107)
- Happiness Hypothesis, The, by Jonathan Haidt - Book SummaryVon EverandHappiness Hypothesis, The, by Jonathan Haidt - Book SummaryBewertung: 4.5 von 5 Sternen4.5/5 (95)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouVon EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNoch keine Bewertungen
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsVon EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsBewertung: 4.5 von 5 Sternen4.5/5 (48)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentVon EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNoch keine Bewertungen
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionVon EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNoch keine Bewertungen
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesVon EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesBewertung: 5 von 5 Sternen5/5 (70)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationVon EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationBewertung: 5 von 5 Sternen5/5 (9)
- It's All Too Much: An Easy Plan for Living a Richer Life with Less StuffVon EverandIt's All Too Much: An Easy Plan for Living a Richer Life with Less StuffBewertung: 4 von 5 Sternen4/5 (232)
- Taking Charge of Adult ADHD, Second Edition: Proven Strategies to Succeed at Work, at Home, and in RelationshipsVon EverandTaking Charge of Adult ADHD, Second Edition: Proven Strategies to Succeed at Work, at Home, and in RelationshipsBewertung: 4.5 von 5 Sternen4.5/5 (25)
- Beyond Thoughts: An Exploration Of Who We Are Beyond Our MindsVon EverandBeyond Thoughts: An Exploration Of Who We Are Beyond Our MindsBewertung: 4.5 von 5 Sternen4.5/5 (7)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeVon EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeBewertung: 5 von 5 Sternen5/5 (560)