Das könnte Ihnen auch gefallen
- Self-Care Self-Efficacy Correlates With Independence in Basic Activities of Daily Living in Individuals With Chronic StrokeDokument7 SeitenSelf-Care Self-Efficacy Correlates With Independence in Basic Activities of Daily Living in Individuals With Chronic StrokeSitti Rosdiana YahyaNoch keine Bewertungen
- Risk Factors Related To Falling in Stroke Patients: A Cross-Sectional StudyDokument3 SeitenRisk Factors Related To Falling in Stroke Patients: A Cross-Sectional StudyZilbran BerontaxNoch keine Bewertungen
- 3 158 1 PBDokument6 Seiten3 158 1 PBViista GiriNoch keine Bewertungen
- High Intensity Exercise For Walking Competency in Individuals With Stroke - A Systematic Review and Meta-AnalysisDokument16 SeitenHigh Intensity Exercise For Walking Competency in Individuals With Stroke - A Systematic Review and Meta-AnalysisSusana RodriguezNoch keine Bewertungen
- Comparison of Mini-Bestest and Dynamic Gait Index For Prediction of Fall Susceptibility in Old IndividualsDokument5 SeitenComparison of Mini-Bestest and Dynamic Gait Index For Prediction of Fall Susceptibility in Old IndividualsElahe SadeqiNoch keine Bewertungen
- Predicting The Probability For Fall Incidence in Stroke Patients Using The Berg Balance ScaleDokument8 SeitenPredicting The Probability For Fall Incidence in Stroke Patients Using The Berg Balance ScaleElahe SadeqiNoch keine Bewertungen
- Correlation Between Self-Efficacy With Activity of Daily Living On Post-Stroke Patients in TMS Clinic RSUD Dr. R. Koesma of TubanDokument7 SeitenCorrelation Between Self-Efficacy With Activity of Daily Living On Post-Stroke Patients in TMS Clinic RSUD Dr. R. Koesma of TubanIsmunandar wahyu KNoch keine Bewertungen
- Stroke Examination and InterventionDokument36 SeitenStroke Examination and InterventionMarikit2012Noch keine Bewertungen
- Functioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenDokument9 SeitenFunctioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenMuhammadMusa47Noch keine Bewertungen
- Physiotherapy Intervention in Alzheimer'sDokument12 SeitenPhysiotherapy Intervention in Alzheimer'sRestu AryaNoch keine Bewertungen
- Acl Rehab ProtocolDokument6 SeitenAcl Rehab ProtocolPricy DevNoch keine Bewertungen
- Review of Effects of Physical Activity On Strength, Balance, Mobility and ADL Performance in Elderly Subjects With DementiaDokument11 SeitenReview of Effects of Physical Activity On Strength, Balance, Mobility and ADL Performance in Elderly Subjects With DementiaAlejandra VasquezNoch keine Bewertungen
- Ms. Neelam Nayak Pranali Mahajan: BackgroundDokument6 SeitenMs. Neelam Nayak Pranali Mahajan: BackgroundYho Ghi GusnandaNoch keine Bewertungen
- Gye Yeop Kim Et Al 2014Dokument6 SeitenGye Yeop Kim Et Al 2014maria.castiyo2002Noch keine Bewertungen
- JIKSH: Jurnal Ilmiah Kesehatan Sandi HusadaDokument6 SeitenJIKSH: Jurnal Ilmiah Kesehatan Sandi HusadaIra ismawatiNoch keine Bewertungen
- Adobe Scan 02 Mar 2023Dokument18 SeitenAdobe Scan 02 Mar 2023ciptakarwanaNoch keine Bewertungen
- Body Weight-Supported Gait Training For Restoration of Walking in People With An Incomplete Spinal Cord Injury: A Systematic ReviewDokument7 SeitenBody Weight-Supported Gait Training For Restoration of Walking in People With An Incomplete Spinal Cord Injury: A Systematic ReviewInterSocial LinkNoch keine Bewertungen
- Headache YesterdayDokument7 SeitenHeadache Yesterdayaahmad87Noch keine Bewertungen
- Stroke 32Dokument8 SeitenStroke 32pokharelriwaj82Noch keine Bewertungen
- Kristenen, NeckmusclebalanceDokument9 SeitenKristenen, NeckmusclebalancePhooi Yee LauNoch keine Bewertungen
- Reliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeDokument8 SeitenReliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeKaniNoch keine Bewertungen
- Daily Living Self Efficacy ScaleDokument8 SeitenDaily Living Self Efficacy Scalespamemail00Noch keine Bewertungen
- Modified Rood's Approach and Ability of Independent Selfcare in Haemorrhagic Stroke Patients of Assam, IndiaDokument6 SeitenModified Rood's Approach and Ability of Independent Selfcare in Haemorrhagic Stroke Patients of Assam, Indianandhini raguNoch keine Bewertungen
- 2020 - Gait RehabilitationDokument8 Seiten2020 - Gait RehabilitationMargarida FonsecaNoch keine Bewertungen
- 1 KowalczykDokument6 Seiten1 KowalczykLuis Diego Verastegui LeguaNoch keine Bewertungen
- Krajewski Et Al, 2018Dokument6 SeitenKrajewski Et Al, 2018Rahmi LubisNoch keine Bewertungen
- Zimmerman 2008Dokument10 SeitenZimmerman 2008jgomezgNoch keine Bewertungen
- The Swedish Occupational Fatigue Inventory in People With Multiple SclerosisDokument7 SeitenThe Swedish Occupational Fatigue Inventory in People With Multiple SclerosisikrambahariNoch keine Bewertungen
- Ijerph 19 15199 v3Dokument13 SeitenIjerph 19 15199 v3soylahijadeunvampiroNoch keine Bewertungen
- 2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacyDokument7 Seiten2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacySM199021Noch keine Bewertungen
- How Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?Dokument6 SeitenHow Often Should Sitting and Rising From A Chair Be Evaluated in Patients With Duchenne Muscular Dystrophy?JoNoch keine Bewertungen
- 10 5923 J Stroke 20170501 01Dokument9 Seiten10 5923 J Stroke 20170501 01Cristian Florin CrasmaruNoch keine Bewertungen
- Effects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisDokument12 SeitenEffects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisNoor KameliaNoch keine Bewertungen
- 10.1093 PTJ Pzac153Dokument13 Seiten10.1093 PTJ Pzac153evelyn.minichNoch keine Bewertungen
- An 2016Dokument10 SeitenAn 2016fernando_a_gonzalezNoch keine Bewertungen
- Assessment of A Disease-Specific Muscular Impairment Rating Scale in Myotonic DystrophyDokument5 SeitenAssessment of A Disease-Specific Muscular Impairment Rating Scale in Myotonic DystrophyLovadi Emese IldikóNoch keine Bewertungen
- ArtikelDokument6 SeitenArtikeljeinzen14Noch keine Bewertungen
- The Effect of Task-Oriented Activities Training On UpperLimbDokument10 SeitenThe Effect of Task-Oriented Activities Training On UpperLimbbagasNoch keine Bewertungen
- Measurement Tools of StrokeDokument42 SeitenMeasurement Tools of StrokeDharam PandeyNoch keine Bewertungen
- 5 - Yadav Sunita. Correlation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDokument19 Seiten5 - Yadav Sunita. Correlation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDr. Krishna N. SharmaNoch keine Bewertungen
- tmp6E6F TMPDokument10 Seitentmp6E6F TMPFrontiersNoch keine Bewertungen
- Jurnal 1Dokument5 SeitenJurnal 1Fila IdieNoch keine Bewertungen
- Research in Developmental DisabilitiesDokument12 SeitenResearch in Developmental DisabilitiesRun CapNoch keine Bewertungen
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodVon EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNoch keine Bewertungen
- Ffects of Physical Exercise On Balance andDokument19 SeitenFfects of Physical Exercise On Balance andAlfiana ApriliaNoch keine Bewertungen
- Stroke RehabilitationDokument10 SeitenStroke RehabilitationPethuel Pomaloy100% (1)
- Lin 2012Dokument9 SeitenLin 2012Luis Briones Lau.LiNoch keine Bewertungen
- Jurnal Srs SkoliosisDokument5 SeitenJurnal Srs SkoliosisDhiny RatuNoch keine Bewertungen
- Effects of Schroth Method and Core Stabilization Exercises On Idiopathic Scoliosis: A Systematic Review and Meta AnalysisDokument12 SeitenEffects of Schroth Method and Core Stabilization Exercises On Idiopathic Scoliosis: A Systematic Review and Meta AnalysisAsmaa SalamaNoch keine Bewertungen
- Gum Mess On 2003Dokument6 SeitenGum Mess On 2003fajarcolzzzNoch keine Bewertungen
- 1471 2318 13 105Dokument13 Seiten1471 2318 13 105ANoch keine Bewertungen
- Leg Exercise: Effect On Reducing Fatigue and Improving Activities of Daily Living For Hemodialysis PatientsDokument9 SeitenLeg Exercise: Effect On Reducing Fatigue and Improving Activities of Daily Living For Hemodialysis PatientsriadesnitaNoch keine Bewertungen
- Effectiveness of Manual Perturbation Exercises inDokument7 SeitenEffectiveness of Manual Perturbation Exercises inSabarie PNoch keine Bewertungen
- Journal of Science and Medicine in SportDokument6 SeitenJournal of Science and Medicine in SportAlvaro FernandoNoch keine Bewertungen
- Jurnal 2 Stroke LinggaDokument9 SeitenJurnal 2 Stroke LinggaLingga Dewi SaraswatiNoch keine Bewertungen
- Rega Sugianto - J120190031 - EJHD Article Review 1Dokument20 SeitenRega Sugianto - J120190031 - EJHD Article Review 1j130235024Noch keine Bewertungen
- Registry of Outcome Measures With MDC 2010Dokument125 SeitenRegistry of Outcome Measures With MDC 2010bdesai48100% (1)
- Stump C Lit Reivew FinalDokument8 SeitenStump C Lit Reivew Finalapi-621438645Noch keine Bewertungen
- The General Function Score: A Useful Tool For Measurement of Physical Disability. Validity and ReliabilityDokument8 SeitenThe General Function Score: A Useful Tool For Measurement of Physical Disability. Validity and ReliabilityLatifatus SirriyahNoch keine Bewertungen
- Exercise Physiology for the Pediatric and Congenital CardiologistVon EverandExercise Physiology for the Pediatric and Congenital CardiologistNoch keine Bewertungen
- Osteoarthritis PDFDokument1 SeiteOsteoarthritis PDFUliuliauliaNoch keine Bewertungen
- Emd166 Slide Acute Coronary PDFDokument40 SeitenEmd166 Slide Acute Coronary PDFUliuliauliaNoch keine Bewertungen
- Manajemen OrganisasiDokument39 SeitenManajemen OrganisasiUliuliauliaNoch keine Bewertungen
- The Effect of Education On Knowledge, Self Management Behaviours and Self Efficacy of Patients With Type 2 DiabetesDokument9 SeitenThe Effect of Education On Knowledge, Self Management Behaviours and Self Efficacy of Patients With Type 2 DiabetesUliuliauliaNoch keine Bewertungen
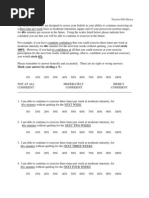
- 100%. However, If You Had No Confidence at All That You Could Exercise at Your ExerciseDokument2 Seiten100%. However, If You Had No Confidence at All That You Could Exercise at Your ExerciseUliuliauliaNoch keine Bewertungen
- Pain Self Efficacy QuestionnaireDokument2 SeitenPain Self Efficacy QuestionnaireUliuliauliaNoch keine Bewertungen
- Music Therapy Sangat Populer Saat Ini. Tapi Pada Saat Ini Jarang Di GunakanDokument6 SeitenMusic Therapy Sangat Populer Saat Ini. Tapi Pada Saat Ini Jarang Di GunakanElfanizar YusandiNoch keine Bewertungen
- Ambulance OperationsDokument36 SeitenAmbulance OperationsUliuliauliaNoch keine Bewertungen
- Attempts: Over Are AnDokument2 SeitenAttempts: Over Are AnSayed AbozeidNoch keine Bewertungen
- Clock Drawing Test PDFDokument6 SeitenClock Drawing Test PDFfissionmailedNoch keine Bewertungen
- Identifying A Cut-Off Point For Normal Mobility: A Comparison of The Timed Up and Go' Test in Community-Dwelling and Institutionalised Elderly WomenDokument6 SeitenIdentifying A Cut-Off Point For Normal Mobility: A Comparison of The Timed Up and Go' Test in Community-Dwelling and Institutionalised Elderly WomenCarolina SandovalNoch keine Bewertungen
- Geriatric Nursing: Feature ArticleDokument5 SeitenGeriatric Nursing: Feature ArticleBryan NguyenNoch keine Bewertungen
- DeliriumDokument12 SeitenDeliriumChrysi TsiouriNoch keine Bewertungen
- Curriculum Resource GuideDokument113 SeitenCurriculum Resource GuideAditya Dana IswaraNoch keine Bewertungen
- Bedridden Elderly: Factors and Risks: August 2020Dokument5 SeitenBedridden Elderly: Factors and Risks: August 2020ammarsalama997Noch keine Bewertungen
- Guidelines For The Falls Risk AssessmentDokument2 SeitenGuidelines For The Falls Risk AssessmentAnonymous tbJ24554Noch keine Bewertungen
- Geriatric SyndromeDokument16 SeitenGeriatric SyndromeJia Jia R'chelNoch keine Bewertungen
- MN Geriatric Nursing - SET2Dokument15 SeitenMN Geriatric Nursing - SET2dila punNoch keine Bewertungen
- Sas 3Dokument3 SeitenSas 3Dummy AccountNoch keine Bewertungen
- 0 The Timed Up and Go TestDokument9 Seiten0 The Timed Up and Go Testapi-593365151Noch keine Bewertungen
- Turquoise Heart Vector Medical BrochureDokument2 SeitenTurquoise Heart Vector Medical BrochureMAUREN DAZANoch keine Bewertungen
- Ageing Prisoners: An Introduction To Geriatric Health-Care Challenges in Correctional FacilitiesDokument24 SeitenAgeing Prisoners: An Introduction To Geriatric Health-Care Challenges in Correctional FacilitiesepraetorianNoch keine Bewertungen
- Hospital Project Proposal PDFDokument15 SeitenHospital Project Proposal PDFSatya Prakash SundramNoch keine Bewertungen
- Elective 2 2019 SyllabusDokument12 SeitenElective 2 2019 SyllabusMaria Rebecca CorazonNoch keine Bewertungen
- Scope of Community Health NursingDokument22 SeitenScope of Community Health NursingEli Zza Koirala85% (13)
- Dementia Types - Symptoms, Diagnosis, Causes, TreatmentsDokument6 SeitenDementia Types - Symptoms, Diagnosis, Causes, TreatmentsRatnaPrasadNalamNoch keine Bewertungen
- Moca Vs MMSEDokument2 SeitenMoca Vs MMSEYw LiuNoch keine Bewertungen
- Resume For LPNDokument8 SeitenResume For LPNafllwwtjo100% (1)
- New BoleanDokument3 SeitenNew BoleanSachi AnandNoch keine Bewertungen
- Geriatrics IntroDokument15 SeitenGeriatrics IntroAnanya KaurNoch keine Bewertungen
- Transitional Care For Older Adults With Chronic Illness - An Integrated ReviewDokument8 SeitenTransitional Care For Older Adults With Chronic Illness - An Integrated ReviewIJAR JOURNALNoch keine Bewertungen
- McMaster University Geriatrics Journal Club - Lecanemab in Early Alzheimers Disease - by ShanojanDokument35 SeitenMcMaster University Geriatrics Journal Club - Lecanemab in Early Alzheimers Disease - by ShanojanDr. Shanojan Thiyagalingam, FRCPC FACPNoch keine Bewertungen
- 3683263752english Annual Report 2010-11Dokument351 Seiten3683263752english Annual Report 2010-11srinivasanaNoch keine Bewertungen
- 2019 - High Levels of Polypharmacy in RheumatoidDokument7 Seiten2019 - High Levels of Polypharmacy in RheumatoidGustavo ResendeNoch keine Bewertungen
- Ageing, Geriatric Syndrome & Anthropometry - Ger.08.11.2021.dsnDokument10 SeitenAgeing, Geriatric Syndrome & Anthropometry - Ger.08.11.2021.dsnyudhi mdNoch keine Bewertungen
- Meeting Nutritional Needs ElderlyDokument25 SeitenMeeting Nutritional Needs ElderlyJustine PlazaNoch keine Bewertungen
- Association Between Frailty and Time Alive and at Home After Cancer Surgery Among Older Adults: A Population-Based AnalysisDokument19 SeitenAssociation Between Frailty and Time Alive and at Home After Cancer Surgery Among Older Adults: A Population-Based AnalysisJuan Camilo SánchezNoch keine Bewertungen
- Australian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientDokument15 SeitenAustralian Dental Journal - 2015 - Ettinger - Treatment Planning Concepts For The Ageing PatientLorri - Ann LamontNoch keine Bewertungen