Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
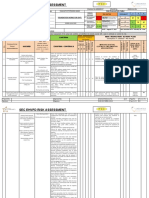
- SEC-EHV-Risk-assesment-form-Rev.-2..Foundation Works For OHTLDokument4 SeitenSEC-EHV-Risk-assesment-form-Rev.-2..Foundation Works For OHTLSn AhsanNoch keine Bewertungen
- Lord of The FliesDokument9 SeitenLord of The FliesKarson TangNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- CH 8: Skeletal System: Includes Bones, Cartilage and LigamentsDokument38 SeitenCH 8: Skeletal System: Includes Bones, Cartilage and LigamentsMightyMouse1379Noch keine Bewertungen
- Comed EVA-HF325, 525 X-Ray - User ManualDokument45 SeitenComed EVA-HF325, 525 X-Ray - User ManualLuis Fernando Garcia S100% (4)
- Marine Perils and P&I Group members: What is coveredDokument17 SeitenMarine Perils and P&I Group members: What is coveredDalilaNoch keine Bewertungen
- Resolution Preliminary InvestigationDokument3 SeitenResolution Preliminary InvestigationJan Lee100% (1)
- Neuroanatomy Questions GuideDokument19 SeitenNeuroanatomy Questions GuideGoNoch keine Bewertungen
- Laryngeal Electromyography Emg Lemg PDFDokument3 SeitenLaryngeal Electromyography Emg Lemg PDFSuprit Sn50% (2)
- Anatomy Base 1Dokument29 SeitenAnatomy Base 1mayna ynaNoch keine Bewertungen
- For Office Use Only Risk AssessmentDokument6 SeitenFor Office Use Only Risk Assessmentbc150Noch keine Bewertungen
- Retinal DetachmentDokument10 SeitenRetinal DetachmentSilpi HamidiyahNoch keine Bewertungen
- Trauma Maksilofasial GuideDokument49 SeitenTrauma Maksilofasial GuideShinta Andi SarasatiNoch keine Bewertungen
- Amls Als Pretest Version 1.11Dokument10 SeitenAmls Als Pretest Version 1.11ArlanosaurusNoch keine Bewertungen
- Upload Required 001Dokument1 SeiteUpload Required 001ArlanosaurusNoch keine Bewertungen
- Covid 19 Checklist Hospitals Preparing Reception Care Coronavirus PatientsDokument8 SeitenCovid 19 Checklist Hospitals Preparing Reception Care Coronavirus Patientsdan_artimof100% (1)
- (TGX) Downloaded From Torrentgalaxy - ToDokument1 Seite(TGX) Downloaded From Torrentgalaxy - ToNeagu Catalin ConstantinNoch keine Bewertungen
- 【Coin Master Free Spins Link Blogspot】$ (2020) $ 【Free Coin Master 400 spins】Coin Master Free Spins And Coins (No Survey)Dokument3 Seiten【Coin Master Free Spins Link Blogspot】$ (2020) $ 【Free Coin Master 400 spins】Coin Master Free Spins And Coins (No Survey)ArlanosaurusNoch keine Bewertungen
- Complete Templates PlanDokument34 SeitenComplete Templates Planmhel20010Noch keine Bewertungen
- Version 2.0 04/08/2020Dokument12 SeitenVersion 2.0 04/08/2020ArlanosaurusNoch keine Bewertungen
- Disease Study WorksheetDokument2 SeitenDisease Study WorksheetwantiNoch keine Bewertungen
- Training Needs Analysis Form for Baguio General Hospital StaffDokument1 SeiteTraining Needs Analysis Form for Baguio General Hospital StaffArlanosaurusNoch keine Bewertungen
- Health Facilities Licensing UpdatesDokument78 SeitenHealth Facilities Licensing Updatespeo geotagNoch keine Bewertungen
- Version 2.0 04/08/2020Dokument12 SeitenVersion 2.0 04/08/2020ArlanosaurusNoch keine Bewertungen
- Estimation of PO2 and FiO2 PDFDokument1 SeiteEstimation of PO2 and FiO2 PDFArlanosaurusNoch keine Bewertungen
- Infectious Diseases and Micro Project Cover SheetDokument3 SeitenInfectious Diseases and Micro Project Cover SheetArlanosaurusNoch keine Bewertungen
- Breathing Ventilation and OxygenationDokument30 SeitenBreathing Ventilation and OxygenationArlanosaurus100% (1)
- TEMS Evaluation Sheet 1.1 - Bag-Valve-MaskDokument1 SeiteTEMS Evaluation Sheet 1.1 - Bag-Valve-MaskArlanosaurusNoch keine Bewertungen
- TTT Orthopaedic InjuriesDokument184 SeitenTTT Orthopaedic InjuriesArlanosaurusNoch keine Bewertungen
- EMS Tuba Pre-Hospital Care Guide - Section 6Dokument4 SeitenEMS Tuba Pre-Hospital Care Guide - Section 6ArlanosaurusNoch keine Bewertungen
- Module D Lesson10 EmergencyDokument7 SeitenModule D Lesson10 EmergencyArlanosaurusNoch keine Bewertungen
- Philippine Military Academy Cadetship Application FormDokument2 SeitenPhilippine Military Academy Cadetship Application FormArlanosaurusNoch keine Bewertungen
- Borrowed TimeDokument6 SeitenBorrowed TimeArlanosaurusNoch keine Bewertungen
- Principles of SplintingDokument1 SeitePrinciples of SplintingArlanosaurusNoch keine Bewertungen
- Pds Rev 2005Dokument4 SeitenPds Rev 2005ArlanosaurusNoch keine Bewertungen
- Emergency Medical Services NC IIDokument154 SeitenEmergency Medical Services NC IIJay Villacorta100% (1)
- Volunteer Sign Up Form: Personal InformationDokument2 SeitenVolunteer Sign Up Form: Personal InformationArlanosaurusNoch keine Bewertungen
- TTT Application FormDokument1 SeiteTTT Application FormArlanosaurusNoch keine Bewertungen
- Learning Style QuestionnaireDokument5 SeitenLearning Style QuestionnaireArlanosaurusNoch keine Bewertungen
- Learning Style QuestionnaireDokument5 SeitenLearning Style QuestionnaireArlanosaurusNoch keine Bewertungen
- Operation Uniform ProposalDokument1 SeiteOperation Uniform ProposalArlanosaurusNoch keine Bewertungen
- He Paid It AllDokument3 SeitenHe Paid It AllArlanosaurusNoch keine Bewertungen
- Application Letter: Download HereDokument1 SeiteApplication Letter: Download HereArlanosaurusNoch keine Bewertungen
- 1 Personal SafetyDokument2 Seiten1 Personal SafetyVladNoch keine Bewertungen
- Types and Causes of HemorrhageDokument26 SeitenTypes and Causes of HemorrhagepriyagidhuNoch keine Bewertungen
- Stulz Cyberrow DX Iom Owr0129aDokument96 SeitenStulz Cyberrow DX Iom Owr0129aBùi LinhNoch keine Bewertungen
- 96-8000L English Mill Operator PDFDokument207 Seiten96-8000L English Mill Operator PDFThomson SimanjuntakNoch keine Bewertungen
- Skin - Structure and Function Flashcards - QuizletDokument5 SeitenSkin - Structure and Function Flashcards - QuizletDani AnyikaNoch keine Bewertungen
- Carpal tunnel syndrome anatomy and treatmentDokument26 SeitenCarpal tunnel syndrome anatomy and treatmentRamzi ShukriNoch keine Bewertungen
- Determining Sex and Race from Skeletal RemainsDokument2 SeitenDetermining Sex and Race from Skeletal RemainsjongreenlikesapplesNoch keine Bewertungen
- Identifying School and Community Resources in Case of Injury or EmergencyDokument29 SeitenIdentifying School and Community Resources in Case of Injury or EmergencyAlyssa AlejandroNoch keine Bewertungen
- Pregnancy ExcerciceDokument2 SeitenPregnancy Excercicetzamarin1Noch keine Bewertungen
- Endodontic Surgery: Incision and DrainageDokument8 SeitenEndodontic Surgery: Incision and DrainageHadoo OolaNoch keine Bewertungen
- Scalp & Skull AnatomyDokument3 SeitenScalp & Skull AnatomyAngel Kim100% (1)
- Sony TV WALL MOUNT Bracket Install GuideDokument321 SeitenSony TV WALL MOUNT Bracket Install GuideRobert-Constantin CristeaNoch keine Bewertungen
- Webster Uretroplastia en 4 Etapas.Dokument13 SeitenWebster Uretroplastia en 4 Etapas.LuisamdNoch keine Bewertungen
- Tourniquet Application During AnesthesiaDokument7 SeitenTourniquet Application During AnesthesiaaksinuNoch keine Bewertungen
- 25 4.3 Connective Tissue Supports and ProtectsDokument17 Seiten25 4.3 Connective Tissue Supports and ProtectsJimmy Jamarolin JacaNoch keine Bewertungen
- Epiglu - Instructions For UseDokument2 SeitenEpiglu - Instructions For Usezeinabhabeeb100% (1)
- Risk Assesment For StudioDokument5 SeitenRisk Assesment For StudioaishahkhanNoch keine Bewertungen
- ( (Think Like A Neurologist) ) 2Dokument61 Seiten( (Think Like A Neurologist) ) 2Mustafa AdelNoch keine Bewertungen