Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Injury Risk Profile and Aging Among Québec FirefightersDokument11 SeitenInjury Risk Profile and Aging Among Québec FirefightersrabodoraaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Teamwork in Operation Room NursingDokument113 SeitenTeamwork in Operation Room NursingrabodoraaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Factors Related To Injury of Shiftworking Fire Fighters in The Northeastern United StatesDokument9 SeitenFactors Related To Injury of Shiftworking Fire Fighters in The Northeastern United Statesrabodoraa100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Cracking Jokes and Crafting SelvesDokument26 SeitenCracking Jokes and Crafting SelvesrabodoraaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Problem Perception and Knowledge Stucture in Expert and Novice Mathematical Problem SolversDokument31 SeitenProblem Perception and Knowledge Stucture in Expert and Novice Mathematical Problem SolversrabodoraaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Slip and Fall Risk Among Firefighters in Relation To Balance, Muscular Capacities and AgeDokument14 SeitenSlip and Fall Risk Among Firefighters in Relation To Balance, Muscular Capacities and AgerabodoraaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Testosterone and The Work of Firefighters Fighting Fires and Delivering Medical CareDokument9 SeitenTestosterone and The Work of Firefighters Fighting Fires and Delivering Medical CarerabodoraaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Injury Risk Profile and Aging Among Québec FirefightersDokument11 SeitenInjury Risk Profile and Aging Among Québec FirefightersrabodoraaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Comparis Posit Negat Experien Antarctic Winter StationDokument27 SeitenComparis Posit Negat Experien Antarctic Winter StationrabodoraaNoch keine Bewertungen
- Development of A Perceptual Hyperthermia Index To Evaluate Heat Strain During Treadmill Exercise PDFDokument10 SeitenDevelopment of A Perceptual Hyperthermia Index To Evaluate Heat Strain During Treadmill Exercise PDFrabodoraaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Journal of Mass EmergenciesDokument117 SeitenJournal of Mass EmergenciesrabodoraaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Influence of Color On Fire Vehicle AccidentsDokument8 SeitenInfluence of Color On Fire Vehicle AccidentsrabodoraaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
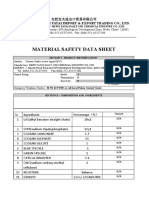
- Soluble OilDokument7 SeitenSoluble OilCarlos SalazarNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- TM 55 1905 242 14Dokument1.001 SeitenTM 55 1905 242 14mercury7k29750Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Ez-10 MSDSDokument5 SeitenEz-10 MSDSMark Evan SalutinNoch keine Bewertungen
- MsdsDokument6 SeitenMsdsRoby SuheriNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Msds CATIONIC D.BASE ACTIVE 18%Dokument5 SeitenMsds CATIONIC D.BASE ACTIVE 18%Alma PustaNoch keine Bewertungen
- DMDHEU PropertiesDokument24 SeitenDMDHEU PropertiesTrầnChíTrungNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Msds CuSO4.5H2ODokument6 SeitenMsds CuSO4.5H2OFebrina Tri NarantiNoch keine Bewertungen
- Eczema and DermatitisDokument7 SeitenEczema and DermatitisDian BaldonadoNoch keine Bewertungen
- Aluminium Potassium SulfateDokument5 SeitenAluminium Potassium SulfatephyphoNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Biolog IDokument38 SeitenBiolog IdedyNoch keine Bewertungen
- Hurst Blue FluidDokument5 SeitenHurst Blue Fluidvince1131Noch keine Bewertungen
- Nu Strip Paint StripperDokument3 SeitenNu Strip Paint StripperJuyta SiahaanNoch keine Bewertungen
- William Boericke Homeopathic Materia MedicaiiDokument592 SeitenWilliam Boericke Homeopathic Materia MedicaiiWilson Bernardes100% (3)
- MiconazoleDokument3 SeitenMiconazoleapi-3797941Noch keine Bewertungen
- Workshop Manual PDFDokument5.126 SeitenWorkshop Manual PDFkevin100% (1)
- Material Safety Data Sheet According To 91/155 ECDokument4 SeitenMaterial Safety Data Sheet According To 91/155 ECvinithaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Ensolv MSDSDokument4 SeitenEnsolv MSDSinfactwayNoch keine Bewertungen
- Msds Fehling BDokument6 SeitenMsds Fehling BndutpesekNoch keine Bewertungen
- MSDS Fertilizer and HerbisidaDokument12 SeitenMSDS Fertilizer and HerbisidaEvi HerawatiNoch keine Bewertungen
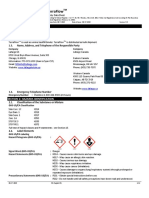
- Lafarge Terraflow en 190617Dokument12 SeitenLafarge Terraflow en 190617Pat AuffretNoch keine Bewertungen
- Usg Cal Seal w60 Gypsum Cement Sds en 52000000037 PDFDokument8 SeitenUsg Cal Seal w60 Gypsum Cement Sds en 52000000037 PDFAMSNoch keine Bewertungen
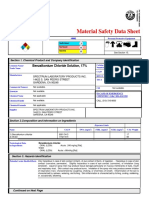
- Benzalkonium Chloride Solution, 17% MSDS - Revision 09-09-08Dokument7 SeitenBenzalkonium Chloride Solution, 17% MSDS - Revision 09-09-08New TubeNoch keine Bewertungen
- SDS CRC Coil CleanerDokument10 SeitenSDS CRC Coil CleanerrudiNoch keine Bewertungen
- JMESTN42353866Dokument7 SeitenJMESTN42353866solomon MorrisonNoch keine Bewertungen
- Msds Cobalt Chloride PDFDokument6 SeitenMsds Cobalt Chloride PDFRizal BahroniNoch keine Bewertungen
- Material Safety Data SheetDokument16 SeitenMaterial Safety Data Sheetaya sofiaNoch keine Bewertungen
- Safety Data Sheet: W. R. Meadows, IncDokument3 SeitenSafety Data Sheet: W. R. Meadows, IncalbertmunozNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Yeast Infection Symptoms in The Belly ButtonDokument4 SeitenYeast Infection Symptoms in The Belly ButtonHIA GS AACNoch keine Bewertungen
- Devcon F - MsdsDokument10 SeitenDevcon F - MsdshamadaNoch keine Bewertungen
- Material Safety Avabentoil EctDokument4 SeitenMaterial Safety Avabentoil Ectfs1640Noch keine Bewertungen