Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Ceux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Dokument1 SeiteCeux1234567890-09876543223456780Pohgcs Xcmepowertyuwed5Wazxnko654Wacvbnkuytresxcvbni76Rdcnmki543345678P .,Mnbvdsq345Teuku IrwandaNoch keine Bewertungen
- Inguinal CanalDokument4 SeitenInguinal CanalspiraldaoNoch keine Bewertungen
- Exam 3 NotesDokument3 SeitenExam 3 NotesStanley ChuNoch keine Bewertungen
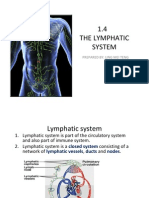
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDokument15 Seiten1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNoch keine Bewertungen
- Animal Morphology (GeoZoo Topics)Dokument5 SeitenAnimal Morphology (GeoZoo Topics)niravhirparaNoch keine Bewertungen
- Our Senses: Seeing, Hearing, and Smelling The WorldDokument63 SeitenOur Senses: Seeing, Hearing, and Smelling The WorldTyler100% (6)
- Musculoskeletal System Lecture NotesDokument169 SeitenMusculoskeletal System Lecture Noteszygote0711578796% (28)
- Chapter 4Dokument7 SeitenChapter 4R LashNoch keine Bewertungen
- January 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelDokument24 SeitenJanuary 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelkirthikaNoch keine Bewertungen
- Abdominal Compartment SyndromeDokument15 SeitenAbdominal Compartment SyndromePierinaNoch keine Bewertungen
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Dokument10 SeitenThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Neurodegenerative Cerebellar AtaxiaDokument26 SeitenNeurodegenerative Cerebellar AtaxiaМилица МилошевићNoch keine Bewertungen
- Science: Quarter 1 - Module 1Dokument10 SeitenScience: Quarter 1 - Module 1RUTH PIANGNoch keine Bewertungen
- Sri Padmavathi Medical College Hospital: APPLICATIONS Are INVITED For The Following Post - 2013-14Dokument3 SeitenSri Padmavathi Medical College Hospital: APPLICATIONS Are INVITED For The Following Post - 2013-14Birupakshya RoutNoch keine Bewertungen
- Management of Clients With Disturbances in OxygenationDokument13 SeitenManagement of Clients With Disturbances in OxygenationClyde CapadnganNoch keine Bewertungen
- The Difference Between Toxic and Nontoxic GoiterDokument2 SeitenThe Difference Between Toxic and Nontoxic GoiterJawad Rehman100% (1)
- C5 - Metabolism and Enzyme Part 1Dokument20 SeitenC5 - Metabolism and Enzyme Part 1Daniel LohNoch keine Bewertungen
- NTSE Stage 1 State Level Model Paper 14Dokument4 SeitenNTSE Stage 1 State Level Model Paper 14AmanNoch keine Bewertungen
- Nutritional Management of High Output Enterocutaneous FistulaDokument2 SeitenNutritional Management of High Output Enterocutaneous FistulaAfra AmiraNoch keine Bewertungen
- Blood TransfusionDokument6 SeitenBlood TransfusionRoxanne Quiñones GelacioNoch keine Bewertungen
- Abdominal SurgeryDokument166 SeitenAbdominal SurgeryIndera VyasNoch keine Bewertungen
- Essential Ayurveda BookDokument196 SeitenEssential Ayurveda BookRoberto89% (9)
- Introduction to MedicineDokument156 SeitenIntroduction to MedicineEshetu BizunehNoch keine Bewertungen
- Nutrition in Plants and AnimalsDokument3 SeitenNutrition in Plants and AnimalsHaris Ur RehmanNoch keine Bewertungen
- Test Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendDokument15 SeitenTest Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendVanessa Martin100% (30)
- Comprehensive Review of Temporal Lobe EpilepsyDokument36 SeitenComprehensive Review of Temporal Lobe Epilepsyyohanes0gadiNoch keine Bewertungen
- BTLDokument60 SeitenBTLCamiNoch keine Bewertungen
- General Zoology SyllabusDokument4 SeitenGeneral Zoology SyllabusNL R Q DO100% (3)
- Comparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemDokument8 SeitenComparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemCentral Asian StudiesNoch keine Bewertungen
- UntitledDokument89 SeitenUntitledVladimir VešovićNoch keine Bewertungen