Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- A 27 Year-Old Woman Woke Up This Morning With Her Eyelids Stuck Together. She Has A Gritty Feeling OnDokument20 SeitenA 27 Year-Old Woman Woke Up This Morning With Her Eyelids Stuck Together. She Has A Gritty Feeling OnUgeshwaran Aristotle ReddyNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- MCEM Anatomy MCQ PDFDokument44 SeitenMCEM Anatomy MCQ PDFUgeshwaran Aristotle Reddy100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- This Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionDokument8 SeitenThis Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionUgeshwaran Aristotle Reddy50% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- MCEM Original Practice MCQs No2Dokument11 SeitenMCEM Original Practice MCQs No2Ugeshwaran Aristotle Reddy100% (2)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Clinical Practice Guidelines 11-18Dokument20 SeitenClinical Practice Guidelines 11-18Feroz RaZa SoomrOoNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Courtney Maxey JonesDokument2 SeitenCourtney Maxey JonesTed BakerNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
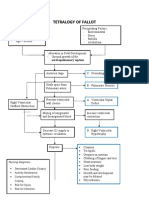
- Concept Map Tetralogy of FallotDokument2 SeitenConcept Map Tetralogy of FallotKarl KiwisNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Heart Sounds:: The Third Sound Is Caused by Vibrations During Passive Filling of The Ventricles With The BloodDokument2 SeitenHeart Sounds:: The Third Sound Is Caused by Vibrations During Passive Filling of The Ventricles With The BloodShmuel BarshalomNoch keine Bewertungen
- Cardiac Risk AssessmentDokument4 SeitenCardiac Risk Assessmentmonir61Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- PPCMDokument7 SeitenPPCMRizki FitriantoNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Medical Surgical Nursing Pre-Test 2 RATIONALEDokument8 SeitenMedical Surgical Nursing Pre-Test 2 RATIONALEBlaine ManiegoNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Lecture III Valvular Heart Diseases and EndocarditisDokument43 SeitenLecture III Valvular Heart Diseases and EndocarditisShahd KhatibNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- FC Cardio (SA) Final Past Papers 1Dokument2 SeitenFC Cardio (SA) Final Past Papers 1matentenNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Calcium Channel Blockers inDokument15 SeitenCalcium Channel Blockers inAnonymous NeRC5JYiSNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
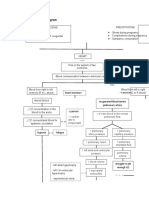
- Path o PhysiologyDokument2 SeitenPath o PhysiologyPotato BroNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- PericarditisDokument29 SeitenPericarditisPavin KumarNoch keine Bewertungen
- Disorders of Cardiac RhythmDokument66 SeitenDisorders of Cardiac RhythmslyfoxkittyNoch keine Bewertungen
- SVT and DengueDokument4 SeitenSVT and Denguefrengki prasNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- RHEUMATIC HEART DISEASE PPT (Autosaved)Dokument44 SeitenRHEUMATIC HEART DISEASE PPT (Autosaved)abid AliNoch keine Bewertungen
- Pediatrics - Michael GrantDokument78 SeitenPediatrics - Michael GrantPappitha RajaNoch keine Bewertungen
- DiltiazemDokument66 SeitenDiltiazemInggar DeozNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- PMR Poster TBI Takotsubo AAP 2010 PosterDokument1 SeitePMR Poster TBI Takotsubo AAP 2010 PosterjuanvelasquezNoch keine Bewertungen
- ESC Guidelines For The Diagnosis and Treatment of Chronic Heart FailureDokument26 SeitenESC Guidelines For The Diagnosis and Treatment of Chronic Heart FailureNareshiman SubramaniamNoch keine Bewertungen
- SDCEP Antibiotic Prophylaxis Summary FlowchartDokument1 SeiteSDCEP Antibiotic Prophylaxis Summary FlowchartMahmoud EladawyNoch keine Bewertungen
- TLC9803 User Manual-258635641Dokument56 SeitenTLC9803 User Manual-258635641sloba.barniNoch keine Bewertungen
- NCLEX Based 1000 MCQs Part-2Dokument12 SeitenNCLEX Based 1000 MCQs Part-2AkashNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Prinsip Dasar Dan Interpretasi EKGDokument44 SeitenPrinsip Dasar Dan Interpretasi EKGFiraNoch keine Bewertungen
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDokument25 SeitenCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHNoch keine Bewertungen
- Pharma Medical Director Cardiology in NYC Resume Ronald HabermanDokument3 SeitenPharma Medical Director Cardiology in NYC Resume Ronald HabermanRonaldHabermanNoch keine Bewertungen
- P07F0502108 Compatibility Chart FASD Rev 08Dokument1 SeiteP07F0502108 Compatibility Chart FASD Rev 08anantasit sirisootNoch keine Bewertungen
- Bhat 2013Dokument5 SeitenBhat 2013Irvin MarcelNoch keine Bewertungen
- ER & CCU ProtocolDokument14 SeitenER & CCU ProtocolatinafansifNoch keine Bewertungen
- (Physio A) ECG (Javier)Dokument4 Seiten(Physio A) ECG (Javier)AliNoch keine Bewertungen
- Angiography Artis One Businesscase Brochure-02018163Dokument4 SeitenAngiography Artis One Businesscase Brochure-02018163TRUONG HOANG DUCNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)