Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- PAAM LecturesDokument167 SeitenPAAM LecturesekyecNoch keine Bewertungen
- Communicable Disease - Community Health NursingDokument49 SeitenCommunicable Disease - Community Health Nursinggelean payod100% (1)
- Medifocus April 2007Dokument61 SeitenMedifocus April 2007Pushpanjali Crosslay HospitalNoch keine Bewertungen
- Noun ClassesDokument51 SeitenNoun ClassesAvrahamNoch keine Bewertungen
- Lou Gehrigs Disease PresentationDokument15 SeitenLou Gehrigs Disease PresentationAdi ParamarthaNoch keine Bewertungen
- Assessment, Northwick ParkDokument2 SeitenAssessment, Northwick ParkMelian Anita100% (1)
- Exercise Prescription GuidelinesDokument9 SeitenExercise Prescription GuidelinesJoshua Arceo100% (2)
- Doctor Charting Guidelines for HPI, Exams and ManagementDokument2 SeitenDoctor Charting Guidelines for HPI, Exams and ManagementMacy Valenciano MacatuggalNoch keine Bewertungen
- Drug StudyDokument5 SeitenDrug StudyinjilbalazoNoch keine Bewertungen
- Mechanical Ventilation Formulas and Norms Flashcards - QuizletDokument8 SeitenMechanical Ventilation Formulas and Norms Flashcards - QuizletAnonymous mNQq7ojNoch keine Bewertungen
- Prepration of The Isolation UnitDokument43 SeitenPrepration of The Isolation UnitGayatri MudliyarNoch keine Bewertungen
- Resurgence of TB linked to increased pneumothoraxDokument5 SeitenResurgence of TB linked to increased pneumothoraxM Tata SuhartaNoch keine Bewertungen
- Waldenstroms Macroglobulinemia (WM) FinalDokument57 SeitenWaldenstroms Macroglobulinemia (WM) FinalnishNoch keine Bewertungen
- GROUP 5-Alzheimer's DiseaseDokument116 SeitenGROUP 5-Alzheimer's Diseasehanna caballoNoch keine Bewertungen
- Tetanus: Andrew Michael Taylor FRCADokument4 SeitenTetanus: Andrew Michael Taylor FRCAILHAM AMIENNoch keine Bewertungen
- Ganz 2006Dokument5 SeitenGanz 2006milicaNoch keine Bewertungen
- Development: J. Russell-Silver DwarfismDokument2 SeitenDevelopment: J. Russell-Silver DwarfismislamawniNoch keine Bewertungen
- Emily BrontëDokument2 SeitenEmily BrontëNadeem AnsariNoch keine Bewertungen
- Febrele HemoragiceDokument21 SeitenFebrele HemoragiceRotaru MihaiNoch keine Bewertungen
- Cleric Spell List D&D 5th EditionDokument9 SeitenCleric Spell List D&D 5th EditionLeandros Mavrokefalos100% (2)
- Delirium and DementiaDokument28 SeitenDelirium and Dementiadr_iswahyudhiNoch keine Bewertungen
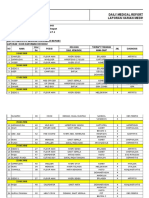
- Daily Medical Report Laporan Harian MedikDokument18 SeitenDaily Medical Report Laporan Harian MedikLehman ManNoch keine Bewertungen
- National Pediatric Nighttime Curriculum on Evaluating and Managing Respiratory Distress in ChildrenDokument18 SeitenNational Pediatric Nighttime Curriculum on Evaluating and Managing Respiratory Distress in ChildrenjerinthomasrajanNoch keine Bewertungen
- Health form parentsDokument1 SeiteHealth form parentsshahidmunirhrNoch keine Bewertungen
- Review of Systems: Skin MusculoskeletalDokument2 SeitenReview of Systems: Skin MusculoskeletalAngelino HernandezNoch keine Bewertungen
- Au Ca2 Psyche Quiz 1 1st Week RatioDokument4 SeitenAu Ca2 Psyche Quiz 1 1st Week RatioYaj CruzadaNoch keine Bewertungen
- Betta Fish Parasite GuideDokument12 SeitenBetta Fish Parasite GuideAngela SoupNoch keine Bewertungen
- Health Declaration Form D02Dokument1 SeiteHealth Declaration Form D02Hizwani ZainalNoch keine Bewertungen
- J.T. Kent's Aphorisms and Precepts on Homoeopathic PhilosophyDokument98 SeitenJ.T. Kent's Aphorisms and Precepts on Homoeopathic PhilosophyYaniv AlgrablyNoch keine Bewertungen
- CVADokument116 SeitenCVAkathy100% (1)