Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Perio 13-14Dokument164 SeitenPerio 13-14priyasargunan50% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Bharathi Notes - Endodontics Questions and Answers-2Dokument24 SeitenBharathi Notes - Endodontics Questions and Answers-2Esha Arora100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Perio 13-14Dokument164 SeitenPerio 13-14priyasargunan50% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- A Clinical Guide To Removable Partial Denture DesignDokument110 SeitenA Clinical Guide To Removable Partial Denture Designd1990d92% (25)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Cast Post N Core For A GD MolarDokument6 SeitenCast Post N Core For A GD MolarDrAvinash NandanNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Perio 13-14Dokument164 SeitenPerio 13-14priyasargunan50% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Polyvinyl Imp. MaterialsDokument7 SeitenPolyvinyl Imp. MaterialsAmar BhochhibhoyaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Techniques of Cleaning Root CanalsDokument12 SeitenTechniques of Cleaning Root CanalsEsha AroraNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Adj 12077Dokument2 SeitenAdj 12077Esha AroraNoch keine Bewertungen
- Adc March 2013 MCQ Part BDokument2 SeitenAdc March 2013 MCQ Part BEsha Arora100% (2)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Gardners MCQDokument244 SeitenGardners MCQEsha Arora60% (10)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- AUS BoardreviewerDokument178 SeitenAUS BoardreviewerEsha Arora33% (3)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Rupi March 2013-1Dokument6 SeitenRupi March 2013-1Esha Arora100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Australian Dental Journal Research Special EditionDokument57 SeitenAustralian Dental Journal Research Special EditionEsha AroraNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Adj 12076Dokument4 SeitenAdj 12076Esha AroraNoch keine Bewertungen
- 2-The Timing of Orthod TXDokument8 Seiten2-The Timing of Orthod TXDoVa XuNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- A Clinical Comparison of The New Attachment Obtained by Guided Tissue Regeneration and Coronally Positioned Flap Techniques in The Management of Human Molar F U R C A Tion DefectsDokument9 SeitenA Clinical Comparison of The New Attachment Obtained by Guided Tissue Regeneration and Coronally Positioned Flap Techniques in The Management of Human Molar F U R C A Tion DefectsEsha AroraNoch keine Bewertungen
- A Clinical Comparison of The New Attachment Obtained by Guided Tissue Regeneration and Coronally Positioned Flap Techniques in The Management of Human Molar F U R C A Tion DefectsDokument9 SeitenA Clinical Comparison of The New Attachment Obtained by Guided Tissue Regeneration and Coronally Positioned Flap Techniques in The Management of Human Molar F U R C A Tion DefectsEsha AroraNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The All-Ceramic, Inlay Supported Xed Partial Denture. Part 3. Experimental Approach For Validating The Nite Element AnalysisDokument8 SeitenThe All-Ceramic, Inlay Supported Xed Partial Denture. Part 3. Experimental Approach For Validating The Nite Element AnalysisEsha AroraNoch keine Bewertungen
- Comparisons of Periodontal Status Pregnant and Non Pregnant WomenDokument0 SeitenComparisons of Periodontal Status Pregnant and Non Pregnant WomenEsha AroraNoch keine Bewertungen
- Comparison of Periosteal Pedicle Graft and Subepithelial Connective Tissue Graft For The Treatment of Gingival Recession DefectsDokument7 SeitenComparison of Periosteal Pedicle Graft and Subepithelial Connective Tissue Graft For The Treatment of Gingival Recession DefectsEsha AroraNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Adc March 2013 MCQ Part BDokument2 SeitenAdc March 2013 MCQ Part BEsha Arora100% (2)
- Prelimin ImpressionsDokument56 SeitenPrelimin ImpressionsEsha AroraNoch keine Bewertungen
- Boucher MCQDokument203 SeitenBoucher MCQEsha Arora65% (23)
- Anxiety GuidelineDokument80 SeitenAnxiety GuidelineEsha AroraNoch keine Bewertungen
- Regenerative EndodonticsDokument7 SeitenRegenerative EndodonticsEsha AroraNoch keine Bewertungen
- Oral Mucosal Diseases Inflammatory Dermtoses, Australian Dental JournalDokument16 SeitenOral Mucosal Diseases Inflammatory Dermtoses, Australian Dental JournalEsha AroraNoch keine Bewertungen
- Australian Dental Journal ArticleDokument6 SeitenAustralian Dental Journal ArticleEsha AroraNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Surgery of The Nasal Cavity - Plastic Surgery KeyDokument14 SeitenSurgery of The Nasal Cavity - Plastic Surgery KeyHossam Elden Helmy HaridyNoch keine Bewertungen
- Nil by Mouth Best Practice and Patient EducationDokument3 SeitenNil by Mouth Best Practice and Patient EducationGrace SimarmataNoch keine Bewertungen
- C Is New India Floater Medi Claim PolicyDokument12 SeitenC Is New India Floater Medi Claim PolicyDeepan ManojNoch keine Bewertungen
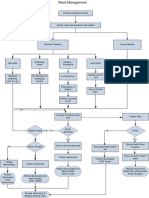
- Ward ManagementDokument1 SeiteWard Managementaman kumar jhaNoch keine Bewertungen
- Complication IntraoperativeDokument5 SeitenComplication IntraoperativeizzatulhasanahNoch keine Bewertungen
- Manual Welch Allyn 62000Dokument186 SeitenManual Welch Allyn 62000mczerpa76010% (1)
- Uptown Magazine June 2009Dokument68 SeitenUptown Magazine June 2009Trimakas100% (6)
- CHAPTER 15 Pain ManagementDokument35 SeitenCHAPTER 15 Pain ManagementIfy OhansonNoch keine Bewertungen
- Federal Law No. 16 of 2007 EngDokument26 SeitenFederal Law No. 16 of 2007 EngZaki AziziNoch keine Bewertungen
- Form 6 New 1 1Dokument2 SeitenForm 6 New 1 1Rosalie HusainNoch keine Bewertungen
- Breast Reconstruction Selected Readings in Plastic SurgeryDokument87 SeitenBreast Reconstruction Selected Readings in Plastic SurgeryJordan LauNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Form 22 ADokument2 SeitenForm 22 AAmrita RaoNoch keine Bewertungen
- Settings Up of OTDokument10 SeitenSettings Up of OTshivaguruNoch keine Bewertungen
- Flexor Tendon InjuriesDokument12 SeitenFlexor Tendon InjuriesFrancis CarterNoch keine Bewertungen
- Somera CaseDokument1 SeiteSomera CaseApril mika ArrocenaNoch keine Bewertungen
- Nursing Care Plan For Cesarean SectionDokument5 SeitenNursing Care Plan For Cesarean SectionJon Gab Paquit85% (33)
- Damage Control Fixation of Displaced Femoral.10Dokument6 SeitenDamage Control Fixation of Displaced Femoral.10Hizkyas KassayeNoch keine Bewertungen
- Self Declaration - Consent Form Poddar Nursing Home and Hospital Before SuregryDokument12 SeitenSelf Declaration - Consent Form Poddar Nursing Home and Hospital Before SuregryRahul PoddarNoch keine Bewertungen
- Essential Client ListDokument5 SeitenEssential Client ListSubhajit SahaNoch keine Bewertungen
- Juan Sumulong High School: English For Academic PurposesDokument59 SeitenJuan Sumulong High School: English For Academic Purposespeter vanderNoch keine Bewertungen
- Lampara Quirurgica-Comen-Serie LDokument6 SeitenLampara Quirurgica-Comen-Serie LDanielRibotNoch keine Bewertungen
- South Korea Life in A Lookist SocietyDokument11 SeitenSouth Korea Life in A Lookist SocietyFlessan MontgomeryNoch keine Bewertungen
- Kat157 PDFDokument50 SeitenKat157 PDFandynightmare97Noch keine Bewertungen
- Surgical Hand AntisepsisDokument19 SeitenSurgical Hand AntisepsisAndy WijayaNoch keine Bewertungen
- Sample Risk Maker Risk Taker GuideDokument18 SeitenSample Risk Maker Risk Taker GuideMilan KukrikaNoch keine Bewertungen
- FessDokument3 SeitenFessMadMariNoch keine Bewertungen
- Understanding Implants in Knee and Hip Replacement - HSSDokument13 SeitenUnderstanding Implants in Knee and Hip Replacement - HSSDavid R. ParejaNoch keine Bewertungen
- Four Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDokument6 SeitenFour Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDevi NingrumNoch keine Bewertungen
- 2015 Trauma ManualDokument165 Seiten2015 Trauma ManualLunaPerfectNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)