Das könnte Ihnen auch gefallen
- Managing Difficult Airway in Obstetric AnesthesiaDokument3 SeitenManaging Difficult Airway in Obstetric AnesthesiaRoman AureliaNoch keine Bewertungen
- Do We Need Other GuidelinesDokument7 SeitenDo We Need Other GuidelinesRoman AureliaNoch keine Bewertungen
- Clinical Practice Guidelines For The Management of The Diffcult AirwayDokument12 SeitenClinical Practice Guidelines For The Management of The Diffcult AirwayRoman AureliaNoch keine Bewertungen
- Anaesthesia For Caesarean Section in Patients With Preterm HELLP SyndromeDokument6 SeitenAnaesthesia For Caesarean Section in Patients With Preterm HELLP SyndromeRoman AureliaNoch keine Bewertungen
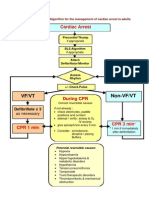
- ASL AlgorithmDokument1 SeiteASL AlgorithmRoman AureliaNoch keine Bewertungen
- Allergic Reactions During AnesthesiaDokument14 SeitenAllergic Reactions During AnesthesiaRoman AureliaNoch keine Bewertungen
- Anaesthetic Considerations For Patients With Pre-Existing NeDokument16 SeitenAnaesthetic Considerations For Patients With Pre-Existing NeRoman AureliaNoch keine Bewertungen
- Allergic Reactions To Anaesthetic DrugsDokument25 SeitenAllergic Reactions To Anaesthetic DrugsRoman AureliaNoch keine Bewertungen
- Rectal and Genital Examination 2Dokument56 SeitenRectal and Genital Examination 22013SecBNoch keine Bewertungen
- Airway Management - Supraglottic Airway PDFDokument4 SeitenAirway Management - Supraglottic Airway PDFPiet Pogen PoelNoch keine Bewertungen
- AmilazemieDokument1 SeiteAmilazemieRoman AureliaNoch keine Bewertungen
- Valori NormaleDokument4 SeitenValori NormaleDragomirescu Ana-cristinaNoch keine Bewertungen
- Ecg in BciDokument7 SeitenEcg in BciRoman AureliaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jin Gui Yao Lue Acupuncture PDFDokument2 SeitenJin Gui Yao Lue Acupuncture PDFJiayiNoch keine Bewertungen
- FAQs on Rabies: Causes, Symptoms, PreventionDokument4 SeitenFAQs on Rabies: Causes, Symptoms, PreventionRonn BautistaNoch keine Bewertungen
- Oxoid UTIDokument2 SeitenOxoid UTISicoe AdrianNoch keine Bewertungen
- Pes 2023Dokument1 SeitePes 2023dr_yasserNoch keine Bewertungen
- Sympathomimetics Drugs REVIEWDokument9 SeitenSympathomimetics Drugs REVIEWLyca SalardaNoch keine Bewertungen
- Alcohol DementiaDokument3 SeitenAlcohol DementiaHenok Moges KassahunNoch keine Bewertungen
- 2014 Pollock British Athletics Muscle Injury Classification - A New Grading SystemDokument6 Seiten2014 Pollock British Athletics Muscle Injury Classification - A New Grading SystemPhysio AcademyNoch keine Bewertungen
- BrastDokument4 SeitenBrastSadishNoch keine Bewertungen
- Em Form NktiDokument7 SeitenEm Form NktiJerico Wendell Gee RubioNoch keine Bewertungen
- Flyer 15th PICU NICU 2024Dokument2 SeitenFlyer 15th PICU NICU 2024rira cassiaNoch keine Bewertungen
- Dermatology Finals (Sept. 2014)Dokument14 SeitenDermatology Finals (Sept. 2014)Paz VidaNoch keine Bewertungen
- Rectal Palpation Harry MomontDokument2 SeitenRectal Palpation Harry MomontMaksar Muhuruna LaodeNoch keine Bewertungen
- Everything You Need to Know About LeukemiaDokument14 SeitenEverything You Need to Know About LeukemiaAkmal HamdanNoch keine Bewertungen
- Arul Kumar An 2013Dokument10 SeitenArul Kumar An 2013Silvana ReyesNoch keine Bewertungen
- Violet Ray Early American Energy MedicineDokument30 SeitenViolet Ray Early American Energy MedicineVerso100% (3)
- Autopsy Reveals Cardiomegaly, Emphysema, CirrhosisDokument5 SeitenAutopsy Reveals Cardiomegaly, Emphysema, CirrhosisInukaicchi TakumichiNoch keine Bewertungen
- Module 13Dokument26 SeitenModule 13Faye Aquino100% (1)
- Day Case Anaesthesia: Andrew Green MBBS, Fracgp GP Anaesthetist ANZCA RegistrarDokument50 SeitenDay Case Anaesthesia: Andrew Green MBBS, Fracgp GP Anaesthetist ANZCA RegistrarSolape Akin-WilliamsNoch keine Bewertungen
- Pathophysiology of Hypertension - The Mosaic Theory and Beyond - JURNALDokument17 SeitenPathophysiology of Hypertension - The Mosaic Theory and Beyond - JURNALidham shadiqNoch keine Bewertungen
- Remdesivir: Remdesivir, Sold Under The Brand Name VekluryDokument16 SeitenRemdesivir: Remdesivir, Sold Under The Brand Name VekluryMd. Shafi NewazNoch keine Bewertungen
- Mombelli 1995Dokument9 SeitenMombelli 1995Ana OrtizNoch keine Bewertungen
- PG Case History Proforma MODIFIEDDokument11 SeitenPG Case History Proforma MODIFIEDSahin mollickNoch keine Bewertungen
- Curs Ia. Anemia AplasticaDokument10 SeitenCurs Ia. Anemia Aplasticaalina2009Noch keine Bewertungen
- HN Iscan, 1997Dokument8 SeitenHN Iscan, 1997Laiana LarussaNoch keine Bewertungen
- Honeymoon Avenue (F#) - BateriaDokument3 SeitenHoneymoon Avenue (F#) - BateriaFranco MarcialNoch keine Bewertungen
- Preparing For A Glucose Tolerance TestDokument3 SeitenPreparing For A Glucose Tolerance Testconnect.rohit85Noch keine Bewertungen
- Facilitator: Mr. Benedict Dwight LepitenDokument26 SeitenFacilitator: Mr. Benedict Dwight LepitenEmmanuelle Soroño AmoresNoch keine Bewertungen
- NCLEX Questions: Nursing Care, Medication Administration & Client EducationDokument3 SeitenNCLEX Questions: Nursing Care, Medication Administration & Client EducationkxviperNoch keine Bewertungen
- Kursus Pementoran Dalam KejururawatanDokument40 SeitenKursus Pementoran Dalam KejururawatanNajlaa RaihanaNoch keine Bewertungen
- AnestesiDokument61 SeitenAnestesiJack Kings QueenNoch keine Bewertungen