Das könnte Ihnen auch gefallen
- Hefler Et Al., 2009Dokument4 SeitenHefler Et Al., 2009Jonathan LucisNoch keine Bewertungen
- Clinical and Morphological Features of Focal AdenomyosisDokument8 SeitenClinical and Morphological Features of Focal AdenomyosisAndika FirmantaraNoch keine Bewertungen
- The Role of Hysteroscopy With Morcellator Without Anesthesia in The Management of Abnormal Uterine BleedingDokument6 SeitenThe Role of Hysteroscopy With Morcellator Without Anesthesia in The Management of Abnormal Uterine Bleedingjorge nnNoch keine Bewertungen
- Cancer - 2000 - Obermair - Does Hysteroscopy Facilitate Tumor Cell DisseminationDokument5 SeitenCancer - 2000 - Obermair - Does Hysteroscopy Facilitate Tumor Cell Disseminationbigefa5107Noch keine Bewertungen
- Recurrence Rate of Endometriomas Following A Laparoscopic CystectomyDokument5 SeitenRecurrence Rate of Endometriomas Following A Laparoscopic CystectomyPutri Tamara DasantosNoch keine Bewertungen
- A Comparative Study of Fine Needle Aspiration Cytology, Trucut Biopsy and Histopathological Examination in Breast LumpsDokument4 SeitenA Comparative Study of Fine Needle Aspiration Cytology, Trucut Biopsy and Histopathological Examination in Breast LumpsIOSRjournalNoch keine Bewertungen
- Cesarean Myomectomy: Kant Anita, Manuja Seema, Pandey RichaDokument3 SeitenCesarean Myomectomy: Kant Anita, Manuja Seema, Pandey RichaAhmad Rahmat Ramadhan TantuNoch keine Bewertungen
- Massa Ovarium Post MenopouseDokument4 SeitenMassa Ovarium Post MenopouseAde Gustina SiahaanNoch keine Bewertungen
- Jurnal 3Dokument5 SeitenJurnal 3Caesar RiefdiNoch keine Bewertungen
- Hysterectomy For Gynecological Indication in Six Medical Facilities in LubumbashiDRC Frequency, Indications, Early Operative ComplicationsDokument11 SeitenHysterectomy For Gynecological Indication in Six Medical Facilities in LubumbashiDRC Frequency, Indications, Early Operative ComplicationsInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Ultrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDokument4 SeitenUltrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDavid Eka PrasetyaNoch keine Bewertungen
- Management of AUB in A Bicornuate Uterus - Endometrial Ablation in A CompDokument1 SeiteManagement of AUB in A Bicornuate Uterus - Endometrial Ablation in A Comptipu42Noch keine Bewertungen
- Evaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsDokument3 SeitenEvaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsNata SanjayaNoch keine Bewertungen
- Computed Tomography in Endometrial CarcinomaDokument5 SeitenComputed Tomography in Endometrial CarcinomasuggaplumNoch keine Bewertungen
- Recurrence of Ovarian Endometrioma After Laparoscopic ExcisionDokument4 SeitenRecurrence of Ovarian Endometrioma After Laparoscopic ExcisionPutri Tamara DasantosNoch keine Bewertungen
- What Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?Dokument6 SeitenWhat Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?dwiagusyuliantoNoch keine Bewertungen
- Lung SOL - Cytology and Histological Correlation in A Tertiary Care CentreDokument7 SeitenLung SOL - Cytology and Histological Correlation in A Tertiary Care CentreIOSRjournalNoch keine Bewertungen
- PDF DIR 378Dokument6 SeitenPDF DIR 378Sidgi BadjriNoch keine Bewertungen
- Rupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. GrudzinskasDokument4 SeitenRupture of Tubal Pregnancy in The Vilnius Population: Pasquale Berlingieri, Grazina Bogdanskiene, Jurgis G. Grudzinskaslilis lestariNoch keine Bewertungen
- A Study On The Knowledge and Management Practices of Hypertension in Establishing A Threshold For Endometrial SamplingDokument8 SeitenA Study On The Knowledge and Management Practices of Hypertension in Establishing A Threshold For Endometrial SamplingGregNoch keine Bewertungen
- Cirugia VaginalDokument4 SeitenCirugia VaginalAna Cristina Gómez RíosNoch keine Bewertungen
- Elkhoury 2015Dokument5 SeitenElkhoury 2015mod_naiveNoch keine Bewertungen
- Medicine: Intrauterine Device Found in An Ovarian TumorDokument5 SeitenMedicine: Intrauterine Device Found in An Ovarian TumorRezky amalia basirNoch keine Bewertungen
- Safety and efficacy of US-guided fiducial marker implantationDokument7 SeitenSafety and efficacy of US-guided fiducial marker implantationAngelito SalinasNoch keine Bewertungen
- Surgical technique of coccygectomy: review of 28 studiesDokument7 SeitenSurgical technique of coccygectomy: review of 28 studiesDiaz RandanilNoch keine Bewertungen
- Residual Breast Tissue After Mastectomy, How Often and Where It Is LocatedDokument11 SeitenResidual Breast Tissue After Mastectomy, How Often and Where It Is LocatedBunga Tri AmandaNoch keine Bewertungen
- Histopathological Correlation of Abnormal Uterine BleedingDokument4 SeitenHistopathological Correlation of Abnormal Uterine BleedingasclepiuspdfsNoch keine Bewertungen
- Detection of Cervical SmearsDokument4 SeitenDetection of Cervical Smearsvyvie89Noch keine Bewertungen
- Diagnosis and Management of Atypical Endometrial HyperplasiaDokument9 SeitenDiagnosis and Management of Atypical Endometrial HyperplasiaagathapradanaNoch keine Bewertungen
- US en EndometritisDokument7 SeitenUS en EndometritisRubí FuerteNoch keine Bewertungen
- Study of Management in Patient With Ectopic Pregnancy: Key WordsDokument3 SeitenStudy of Management in Patient With Ectopic Pregnancy: Key WordsparkfishyNoch keine Bewertungen
- Lymph Nodes Esophageal Cancer Staging: Improved Accuracy by Endoscopic Ultrasound of CeliacDokument5 SeitenLymph Nodes Esophageal Cancer Staging: Improved Accuracy by Endoscopic Ultrasound of CeliacPoonam JoshiNoch keine Bewertungen
- 0068KJR - KJR 5 39Dokument8 Seiten0068KJR - KJR 5 39Louis HadiyantoNoch keine Bewertungen
- Amniocentesis Results and Retrospective Analysis Performed in The University ClinicDokument6 SeitenAmniocentesis Results and Retrospective Analysis Performed in The University ClinicCindy Denti PratikasariNoch keine Bewertungen
- Transvaginal MorcellationDokument8 SeitenTransvaginal Morcellationsanjayb1976gmailcomNoch keine Bewertungen
- Transvaginal myomectomy with screw tractionDokument5 SeitenTransvaginal myomectomy with screw tractionWillis WiNoch keine Bewertungen
- Study of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsDokument5 SeitenStudy of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsArvind Vashi AroraNoch keine Bewertungen
- Pi Is 0020729214001040Dokument5 SeitenPi Is 0020729214001040Nurul AiniNoch keine Bewertungen
- 3 PBDokument6 Seiten3 PBAulia Rizqi MulyaniNoch keine Bewertungen
- Importance of Intraoperative-Touch Imprint Cytology in The Diagnosis of Neoplastic Lesions of Breast.Dokument8 SeitenImportance of Intraoperative-Touch Imprint Cytology in The Diagnosis of Neoplastic Lesions of Breast.IOSRjournalNoch keine Bewertungen
- Jurnal Fistolotomi Vs FistulektomiDokument8 SeitenJurnal Fistolotomi Vs FistulektomiAndriati Nadhila100% (1)
- Surgical Outcome of Genito Urinary Fistula - RayazDokument3 SeitenSurgical Outcome of Genito Urinary Fistula - RayazRiaz Ahmed ChaudhryNoch keine Bewertungen
- Art 20177509Dokument4 SeitenArt 20177509Jashashree SaikiaNoch keine Bewertungen
- 03 JCR 004 Rajendra EndometrialDokument4 Seiten03 JCR 004 Rajendra EndometrialReza HidayatNoch keine Bewertungen
- Cancer de MamaDokument11 SeitenCancer de MamaIng SánchezNoch keine Bewertungen
- Van Dongen Et Al., 2006Dokument5 SeitenVan Dongen Et Al., 2006Jonathan LucisNoch keine Bewertungen
- Clinical and Morphological Features of Uterine FibroidDokument7 SeitenClinical and Morphological Features of Uterine FibroidCentral Asian StudiesNoch keine Bewertungen
- Bladder Calculus Resulting From The Migration of An IntrauterineDokument8 SeitenBladder Calculus Resulting From The Migration of An IntrauterineFabrien Hein WillemNoch keine Bewertungen
- Abdominal Radical Trachelectomy: A Romanian SeriesDokument5 SeitenAbdominal Radical Trachelectomy: A Romanian SeriesPanuta AndrianNoch keine Bewertungen
- 10.1007@s00404 009 1290 yDokument5 Seiten10.1007@s00404 009 1290 yAnonymous g1hIPZNoch keine Bewertungen
- Large Anechogenic "Holes" in The Uterus: The Utility of Contextual Combination of Ultrasound and HysterosDokument3 SeitenLarge Anechogenic "Holes" in The Uterus: The Utility of Contextual Combination of Ultrasound and HysterosBOHR International Journal on GynaecologyNoch keine Bewertungen
- Ijcem0007 1366Dokument4 SeitenIjcem0007 1366Ratih Kusuma DewiNoch keine Bewertungen
- Laparoscopic Myomectomy in Patients With Uterine Myomas Associated With InfertilityDokument9 SeitenLaparoscopic Myomectomy in Patients With Uterine Myomas Associated With Infertilitysanta_pangaribuan_1Noch keine Bewertungen
- Ajr 10 4865Dokument6 SeitenAjr 10 4865ChavdarNoch keine Bewertungen
- Article IJGCP 118Dokument3 SeitenArticle IJGCP 118Jessica MarianoNoch keine Bewertungen
- J Neurosurg Pediatr Article p52Dokument10 SeitenJ Neurosurg Pediatr Article p52Audhrey BNoch keine Bewertungen
- Laparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerDokument7 SeitenLaparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerHari NugrohoNoch keine Bewertungen
- 4083 15383 1 PBDokument5 Seiten4083 15383 1 PBAljoieRoseNoch keine Bewertungen
- Case Studies of Postoperative Complications after Digestive SurgeryVon EverandCase Studies of Postoperative Complications after Digestive SurgeryNoch keine Bewertungen
- 75178347Dokument5 Seiten75178347Ana Di JayaNoch keine Bewertungen
- HydrotubationDokument4 SeitenHydrotubationAna Di Jaya100% (1)
- Renu GargDokument3 SeitenRenu GargAna Di JayaNoch keine Bewertungen
- Case Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaDokument4 SeitenCase Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaAna Di JayaNoch keine Bewertungen
- Journal of Medical Case ReportsDokument4 SeitenJournal of Medical Case ReportsAna Di JayaNoch keine Bewertungen
- HydrotubationDokument4 SeitenHydrotubationAna Di Jaya100% (1)
- Leiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaDokument5 SeitenLeiomyoma and Rhabdomyoma of The Vagina Vaginal MyomaAna Di JayaNoch keine Bewertungen
- Hypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryDokument4 SeitenHypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryAna Di JayaNoch keine Bewertungen
- 2 Pathogenesis TukakLambungDokument30 Seiten2 Pathogenesis TukakLambungAna Di JayaNoch keine Bewertungen
- Viral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementDokument12 SeitenViral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementAna Di JayaNoch keine Bewertungen
- Efficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialDokument5 SeitenEfficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialAna Di JayaNoch keine Bewertungen
- The Early Prevention of Stroke Heart Attack Perki SMG 05Dokument38 SeitenThe Early Prevention of Stroke Heart Attack Perki SMG 05Ana Di JayaNoch keine Bewertungen
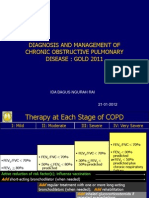
- Rountable Copd Jan 2012Dokument71 SeitenRountable Copd Jan 2012Ana Di JayaNoch keine Bewertungen
- Pengobatan Pada Tiap KomplikasiDokument6 SeitenPengobatan Pada Tiap KomplikasiAna Di JayaNoch keine Bewertungen
- Who Guidlines Pregnancy Woman 2010 PDFDokument117 SeitenWho Guidlines Pregnancy Woman 2010 PDFAna Di JayaNoch keine Bewertungen
- Case of A Woman With Cough and Lung Nodule PDFDokument9 SeitenCase of A Woman With Cough and Lung Nodule PDFAna Di JayaNoch keine Bewertungen
- Cotrimoxazole Profilaxis Hiv Who Guidlines PDFDokument68 SeitenCotrimoxazole Profilaxis Hiv Who Guidlines PDFAna Di JayaNoch keine Bewertungen
- WHO Dengue Guidelines 2013Dokument160 SeitenWHO Dengue Guidelines 2013Jason MirasolNoch keine Bewertungen
- Case of Impaired Renal Funtion PDFDokument1 SeiteCase of Impaired Renal Funtion PDFAna Di JayaNoch keine Bewertungen
- Vol361and2topic04 PDFDokument6 SeitenVol361and2topic04 PDFAna Di JayaNoch keine Bewertungen
- Case of A Womenwith Acute Onset of Chest Pain PDFDokument9 SeitenCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaNoch keine Bewertungen
- Case of Bladder Carcinoma PDFDokument9 SeitenCase of Bladder Carcinoma PDFAna Di JayaNoch keine Bewertungen
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDokument8 SeitenCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaNoch keine Bewertungen
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDokument8 SeitenCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaNoch keine Bewertungen
- Case of A Woman With Obesity, DM An Hypertension PDFDokument10 SeitenCase of A Woman With Obesity, DM An Hypertension PDFAna Di JayaNoch keine Bewertungen
- Case of A Womenwith Acute Onset of Chest Pain PDFDokument9 SeitenCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaNoch keine Bewertungen
- Case of Bladder Carcinoma PDFDokument9 SeitenCase of Bladder Carcinoma PDFAna Di JayaNoch keine Bewertungen
- Case Report .Hepatic Failure PDFDokument4 SeitenCase Report .Hepatic Failure PDFAna Di JayaNoch keine Bewertungen
- Case of Boy With Slowing Growth, Delayed Puberty PDFDokument11 SeitenCase of Boy With Slowing Growth, Delayed Puberty PDFAna Di JayaNoch keine Bewertungen
- Degrees of Comparison: When We Compare Two Nouns: Comparative. When We Compare Three or More Nouns: SuperlativeDokument6 SeitenDegrees of Comparison: When We Compare Two Nouns: Comparative. When We Compare Three or More Nouns: SuperlativeMerlina AryantiNoch keine Bewertungen
- Proforma Invoice: DescriptionDokument3 SeitenProforma Invoice: Descriptionanon-690278Noch keine Bewertungen
- 4mb1 02r Que 20220608Dokument32 Seiten4mb1 02r Que 20220608M.A. HassanNoch keine Bewertungen
- Future War in Cities Alice Hills PDFDokument5 SeitenFuture War in Cities Alice Hills PDFazardarioNoch keine Bewertungen
- Canary TreatmentDokument117 SeitenCanary TreatmentRam KLNoch keine Bewertungen
- Biometric SecurityDokument495 SeitenBiometric SecurityPlay100% (1)
- 797B Commissioning Guidebook 07 (Procesos)Dokument65 Seiten797B Commissioning Guidebook 07 (Procesos)wilmerNoch keine Bewertungen
- Tchaikovsky Piano Concerto 1Dokument2 SeitenTchaikovsky Piano Concerto 1arno9bear100% (2)
- Express VPN Activation CodeDokument5 SeitenExpress VPN Activation CodeButler49JuulNoch keine Bewertungen
- Final Reflective Essay by Georgi ShopovDokument7 SeitenFinal Reflective Essay by Georgi ShopovMd Siddique UllahNoch keine Bewertungen
- Pakistan Affairs Current Affairs 2016 MCQSDokument3 SeitenPakistan Affairs Current Affairs 2016 MCQSMuhammad MudassarNoch keine Bewertungen
- Big Data, Consumer Analytics, and The Transformation of MarketingDokument17 SeitenBig Data, Consumer Analytics, and The Transformation of MarketingPeyush NeneNoch keine Bewertungen
- Explosive Loading of Engineering Structures PDFDokument2 SeitenExplosive Loading of Engineering Structures PDFBillNoch keine Bewertungen
- Construction Internship ReportDokument8 SeitenConstruction Internship ReportDreaminnNoch keine Bewertungen
- Motor Operated ValveDokument6 SeitenMotor Operated ValveYosses Sang NahkodaNoch keine Bewertungen
- Airbus Reference Language AbbreviationsDokument66 SeitenAirbus Reference Language Abbreviations862405Noch keine Bewertungen
- CONTACT DETAILS HC JUDGES LIBRARIESDokument4 SeitenCONTACT DETAILS HC JUDGES LIBRARIESSHIVAM BHATTACHARYANoch keine Bewertungen
- Chenab Railway Bridge Project ReportDokument50 SeitenChenab Railway Bridge Project ReportPreet Chahal100% (1)
- Raj Priya Civil Court Clerk FinalDokument1 SeiteRaj Priya Civil Court Clerk FinalRaj KamalNoch keine Bewertungen
- Securifire 1000-ExtractedDokument2 SeitenSecurifire 1000-ExtractedWilkeey EstrellanesNoch keine Bewertungen
- KEC115/6/7x: Ac Generator Short Circuit and Over Current GuardDokument4 SeitenKEC115/6/7x: Ac Generator Short Circuit and Over Current GuardRN NNoch keine Bewertungen
- Arsh Final Project ReportDokument65 SeitenArsh Final Project Report720 Manvir SinghNoch keine Bewertungen
- Crio - Copy Business Operations - Case Study AssignmentDokument3 SeitenCrio - Copy Business Operations - Case Study Assignmentvaishnawnikhil3Noch keine Bewertungen
- Present Perfect.Dokument1 SeitePresent Perfect.Leidy DiazNoch keine Bewertungen
- Site AnalysisDokument15 SeitenSite Analysismaanik005Noch keine Bewertungen
- Alice in ChainsDokument18 SeitenAlice in ChainsmexicolaNoch keine Bewertungen
- PENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIDokument15 SeitenPENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIRizky Hizrah WumuNoch keine Bewertungen
- Candida by Shaw, George Bernard, 1856-1950Dokument61 SeitenCandida by Shaw, George Bernard, 1856-1950Gutenberg.orgNoch keine Bewertungen
- Berserker - Lifting Wood and Stone Like A Viking Strongman Bodybuilding Functional StrengthDokument10 SeitenBerserker - Lifting Wood and Stone Like A Viking Strongman Bodybuilding Functional Strengthluciferr71Noch keine Bewertungen
- Parts of A Computer With Their FunctionsDokument19 SeitenParts of A Computer With Their FunctionsJaried SumbaNoch keine Bewertungen