Das könnte Ihnen auch gefallen
- 10 1016@j Bpobgyn 2015 11 014Dokument17 Seiten10 1016@j Bpobgyn 2015 11 014Marco Julcamoro AsencioNoch keine Bewertungen
- Uterine MyomaDokument15 SeitenUterine Myomaanon_302623176100% (1)
- Fibro AdenomaDokument12 SeitenFibro AdenomaRahman Az ZamNoch keine Bewertungen
- LI 1 AdenomyosisDokument4 SeitenLI 1 AdenomyosisyasminNoch keine Bewertungen
- Anterior Vaginal Wall Mass Miicking CystoceleDokument4 SeitenAnterior Vaginal Wall Mass Miicking CystoceleDar ADNoch keine Bewertungen
- An Unusual Localization of Leiomyoma: Vaginal LeiomyomaDokument4 SeitenAn Unusual Localization of Leiomyoma: Vaginal Leiomyomaistiana sariNoch keine Bewertungen
- Giant Uterine Leiomyoma - Case Report and Review of LiteratureDokument3 SeitenGiant Uterine Leiomyoma - Case Report and Review of LiteratureMan ManuelNoch keine Bewertungen
- Uterine Fibroids (Leiomyomas) - Differentiating Fibroids From Uterine Sarcomas - UpToDateDokument31 SeitenUterine Fibroids (Leiomyomas) - Differentiating Fibroids From Uterine Sarcomas - UpToDateCristinaCaprosNoch keine Bewertungen
- Makalah Rule of Ultrasound in Management of Uterine LeiomyomaDokument23 SeitenMakalah Rule of Ultrasound in Management of Uterine LeiomyomaKristabella GianinaNoch keine Bewertungen
- Myoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDokument3 SeitenMyoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDiane MargretNoch keine Bewertungen
- 10 18017-Iuitfd 308495-296849Dokument3 Seiten10 18017-Iuitfd 308495-296849asshagab04Noch keine Bewertungen
- Uterine Myoma, Myomectomy and Minimally Invasive TreatmentsVon EverandUterine Myoma, Myomectomy and Minimally Invasive TreatmentsNoch keine Bewertungen
- Keywords: Endometrial Polyp, Endometrioma, Ovarian Cyst, Ovarian Dermoid, PelvicDokument13 SeitenKeywords: Endometrial Polyp, Endometrioma, Ovarian Cyst, Ovarian Dermoid, PelvicWarrodNoch keine Bewertungen
- Case ReportDokument5 SeitenCase ReportLifia VirginiaNoch keine Bewertungen
- A Case of Giant Uterine Fibroid in A Toung WomanDokument5 SeitenA Case of Giant Uterine Fibroid in A Toung WomanTETINOUNoch keine Bewertungen
- Ovarian Fibroma Presents As Uterine Leiomyoma in A 61-Year-Old Female A Case StudyDokument7 SeitenOvarian Fibroma Presents As Uterine Leiomyoma in A 61-Year-Old Female A Case StudyBagus Tri WahyudiNoch keine Bewertungen
- 2.female Genital System IIDokument70 Seiten2.female Genital System IIأسود / BlackNoch keine Bewertungen
- LeiomiomaDokument10 SeitenLeiomiomasirohNoch keine Bewertungen
- Adenomyosis and Infertility - RBMDokument12 SeitenAdenomyosis and Infertility - RBMRika EffendyNoch keine Bewertungen
- EndometriosisDokument5 SeitenEndometriosisLok100% (2)
- Case Study-Endometrial PyometraDokument7 SeitenCase Study-Endometrial Pyometrasimbarashe tangwadzanaNoch keine Bewertungen
- Endocervical PolypDokument2 SeitenEndocervical PolypRez007Noch keine Bewertungen
- Uterine LeiomyomaDokument57 SeitenUterine LeiomyomaRomy Mansour100% (2)
- 2.2 Gyn Pathology OvaryDokument0 Seiten2.2 Gyn Pathology OvarydinapurpleloversNoch keine Bewertungen
- What Is Leiomyoma of The UterusDokument16 SeitenWhat Is Leiomyoma of The Uterusjasper pachingelNoch keine Bewertungen
- From The Archives of The AFIP: Endometriosis: Radiologic-Pathologic CorrelationDokument24 SeitenFrom The Archives of The AFIP: Endometriosis: Radiologic-Pathologic Correlation104022432 104a-Noch keine Bewertungen
- Mixed Müllerian Tumor of UterusDokument3 SeitenMixed Müllerian Tumor of UterusInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- ADENOMYOSISDokument5 SeitenADENOMYOSISdoddydrNoch keine Bewertungen
- Disgerminom OvarianDokument7 SeitenDisgerminom OvarianIfrim MihaelaNoch keine Bewertungen
- PathologyDokument47 SeitenPathologySubburaj Thiruvengadam100% (1)
- Uterine L'eiomyosarcomaDokument4 SeitenUterine L'eiomyosarcomaEldimson BermudoNoch keine Bewertungen
- Uterine Leiomyoma in An Adolescent Female: Case ReportDokument3 SeitenUterine Leiomyoma in An Adolescent Female: Case Reportdr.putra888Noch keine Bewertungen
- Refleksi Kasus Mioma UteriDokument18 SeitenRefleksi Kasus Mioma Uterimichelle1945Noch keine Bewertungen
- Refrat Rsop SarcomaDokument20 SeitenRefrat Rsop Sarcomasweet lilyNoch keine Bewertungen
- 2 Ovarian Cyst UG4-Dr AllanDokument13 Seiten2 Ovarian Cyst UG4-Dr AllanAza BabanNoch keine Bewertungen
- Uterine Sarcomas: Nomonde Mbatani - Alexander B. Olawaiye - Jaime PratDokument8 SeitenUterine Sarcomas: Nomonde Mbatani - Alexander B. Olawaiye - Jaime PratMarco Julcamoro AsencioNoch keine Bewertungen
- Benign and Malignat Ovarian TumorsDokument67 SeitenBenign and Malignat Ovarian TumorsZEMENAY TRUNEHNoch keine Bewertungen
- UPTODATE - MIOMA - Epidemiology, Clinical Manifestations, Diagnosis, and Natural History of Uterine Leiomyomas (Fibroids)Dokument20 SeitenUPTODATE - MIOMA - Epidemiology, Clinical Manifestations, Diagnosis, and Natural History of Uterine Leiomyomas (Fibroids)Gaby FloresNoch keine Bewertungen
- EndometrisisDokument10 SeitenEndometrisisAmmarNoch keine Bewertungen
- Smooth Muscle Tumor of Vulva With Uncertain Malignant PotentialDokument4 SeitenSmooth Muscle Tumor of Vulva With Uncertain Malignant PotentialmajoNoch keine Bewertungen
- Jurnal Polip EndometriumDokument4 SeitenJurnal Polip EndometriumNamira AmmarinNoch keine Bewertungen
- LP NokDokument20 SeitenLP NokGracia Ayu ChristinaNoch keine Bewertungen
- Benign Lesions of The OvariesDokument12 SeitenBenign Lesions of The OvariesdocjosmaNoch keine Bewertungen
- Case Report PathoDokument3 SeitenCase Report PathoZak KazNoch keine Bewertungen
- Uterine Fibroids PDFDokument3 SeitenUterine Fibroids PDFmervat_aastNoch keine Bewertungen
- Vaginal LeiomyomaDokument1 SeiteVaginal LeiomyomaMounika DevathiNoch keine Bewertungen
- Endometriosis at Caesarian Section Scar: Khalifa Al-JabriDokument2 SeitenEndometriosis at Caesarian Section Scar: Khalifa Al-JabriJuan SetiajiNoch keine Bewertungen
- Successful Use of Laparoscopic Myomectomy To Remove A Giant Uterine Myoma A Case ReportDokument4 SeitenSuccessful Use of Laparoscopic Myomectomy To Remove A Giant Uterine Myoma A Case ReportnicabiNoch keine Bewertungen
- A Giant Juvenile Fibroadenoma of BreastDokument2 SeitenA Giant Juvenile Fibroadenoma of BreastIOSRjournalNoch keine Bewertungen
- Benign Neoplasms of The Sexual Organs of A WomanDokument14 SeitenBenign Neoplasms of The Sexual Organs of A WomanArooj AshrafNoch keine Bewertungen
- Retroperitoneal Leiomyoma of Gynecologic Type: A Case Report and Review of The LiteratureDokument5 SeitenRetroperitoneal Leiomyoma of Gynecologic Type: A Case Report and Review of The LiteratureIJAR JOURNALNoch keine Bewertungen
- Myoma Case StudyDokument2 SeitenMyoma Case StudyKristine CastilloNoch keine Bewertungen
- 11 - Benign Gynecologic TumorsDokument61 Seiten11 - Benign Gynecologic TumorsDevy Eryn TobingNoch keine Bewertungen
- 16.uterine Disorders (B.m.a)Dokument35 Seiten16.uterine Disorders (B.m.a)Jimmy MainaNoch keine Bewertungen
- Alternativesto Hysterectomy: Management of Uterine FibroidsDokument17 SeitenAlternativesto Hysterectomy: Management of Uterine FibroidsMarco Julcamoro AsencioNoch keine Bewertungen
- Myoma in Necrobiosis and PregnancyDokument2 SeitenMyoma in Necrobiosis and PregnancyInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Ultrasound in Obstet Gyne - 2018 - Van Den Bosch - Sonographic Classification and Reporting System For DiagnosingDokument7 SeitenUltrasound in Obstet Gyne - 2018 - Van Den Bosch - Sonographic Classification and Reporting System For DiagnosingGraceAnnSanjorjoNoch keine Bewertungen
- Benign Ovarian TumourDokument45 SeitenBenign Ovarian Tumourahmed shorshNoch keine Bewertungen
- AdenomyosisDokument16 SeitenAdenomyosisWiwik'RatnaSariPratiwi'100% (2)
- 75178347Dokument5 Seiten75178347Ana Di JayaNoch keine Bewertungen
- A Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumDokument4 SeitenA Pilot Evaluation of Saline Sonohysterography For Postmenopausal Bleeding With Thickened EndometriumAna Di JayaNoch keine Bewertungen
- Renu GargDokument3 SeitenRenu GargAna Di JayaNoch keine Bewertungen
- HydrotubationDokument4 SeitenHydrotubationAna Di Jaya100% (1)
- Case Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaDokument4 SeitenCase Report: Vaginal Myomectomy For A Thirteen-Centimeter Anterior MyomaAna Di JayaNoch keine Bewertungen
- Journal of Medical Case ReportsDokument4 SeitenJournal of Medical Case ReportsAna Di JayaNoch keine Bewertungen
- HydrotubationDokument4 SeitenHydrotubationAna Di Jaya100% (1)
- Efficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialDokument5 SeitenEfficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialAna Di JayaNoch keine Bewertungen
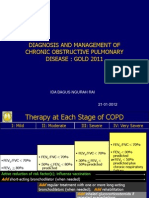
- Rountable Copd Jan 2012Dokument71 SeitenRountable Copd Jan 2012Ana Di JayaNoch keine Bewertungen
- Viral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementDokument12 SeitenViral Encephalitis: Etiology, Clinical Features, Diagnosis and ManagementAna Di JayaNoch keine Bewertungen
- Pengobatan Pada Tiap KomplikasiDokument6 SeitenPengobatan Pada Tiap KomplikasiAna Di JayaNoch keine Bewertungen
- Hypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryDokument4 SeitenHypovolemic Shock Due To Massive Edema of A Pedunculated Uterine Myoma After DeliveryAna Di JayaNoch keine Bewertungen
- Cotrimoxazole Profilaxis Hiv Who Guidlines PDFDokument68 SeitenCotrimoxazole Profilaxis Hiv Who Guidlines PDFAna Di JayaNoch keine Bewertungen
- Who Guidlines Pregnancy Woman 2010 PDFDokument117 SeitenWho Guidlines Pregnancy Woman 2010 PDFAna Di JayaNoch keine Bewertungen
- Vol361and2topic04 PDFDokument6 SeitenVol361and2topic04 PDFAna Di JayaNoch keine Bewertungen
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDokument8 SeitenCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaNoch keine Bewertungen
- WHO Dengue Guidelines 2013Dokument160 SeitenWHO Dengue Guidelines 2013Jason MirasolNoch keine Bewertungen
- The Early Prevention of Stroke Heart Attack Perki SMG 05Dokument38 SeitenThe Early Prevention of Stroke Heart Attack Perki SMG 05Ana Di JayaNoch keine Bewertungen
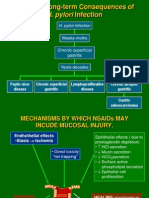
- 2 Pathogenesis TukakLambungDokument30 Seiten2 Pathogenesis TukakLambungAna Di JayaNoch keine Bewertungen
- Case of A Womenwith Acute Onset of Chest Pain PDFDokument9 SeitenCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaNoch keine Bewertungen
- Case of A Womenwith Acute Onset of Chest Pain PDFDokument9 SeitenCase of A Womenwith Acute Onset of Chest Pain PDFAna Di JayaNoch keine Bewertungen
- Case of A Woman With Cough and Lung Nodule PDFDokument9 SeitenCase of A Woman With Cough and Lung Nodule PDFAna Di JayaNoch keine Bewertungen
- Case of A Woman With Obesity, DM An Hypertension PDFDokument10 SeitenCase of A Woman With Obesity, DM An Hypertension PDFAna Di JayaNoch keine Bewertungen
- Case of Bladder Carcinoma PDFDokument9 SeitenCase of Bladder Carcinoma PDFAna Di JayaNoch keine Bewertungen
- Case of Boy With Slowing Growth, Delayed Puberty PDFDokument11 SeitenCase of Boy With Slowing Growth, Delayed Puberty PDFAna Di JayaNoch keine Bewertungen
- Case of Adrenal Nodule in A 59 Yrs Old Women PDFDokument8 SeitenCase of Adrenal Nodule in A 59 Yrs Old Women PDFAna Di JayaNoch keine Bewertungen
- Case of Impaired Renal Funtion PDFDokument1 SeiteCase of Impaired Renal Funtion PDFAna Di JayaNoch keine Bewertungen
- Case of Bladder Carcinoma PDFDokument9 SeitenCase of Bladder Carcinoma PDFAna Di JayaNoch keine Bewertungen
- Case Report .Hepatic Failure PDFDokument4 SeitenCase Report .Hepatic Failure PDFAna Di JayaNoch keine Bewertungen
- Kenya FGM PregnancyDokument65 SeitenKenya FGM Pregnancygeorgeloto12Noch keine Bewertungen
- Sexual IntercourseDokument26 SeitenSexual Intercoursenathan100% (2)
- Chapter 12 - Slides - 350Dokument39 SeitenChapter 12 - Slides - 350Diana MamaticNoch keine Bewertungen
- Postpartum ComplicationsDokument15 SeitenPostpartum Complicationspadmja4purohitNoch keine Bewertungen
- Human SexualityDokument11 SeitenHuman Sexualitylanilyn aquinoNoch keine Bewertungen
- Female Sexual Dysfunction-1Dokument7 SeitenFemale Sexual Dysfunction-1Risky SetiawanNoch keine Bewertungen
- Dyspareunia in Gynaecological Practice: EpidemiologyDokument7 SeitenDyspareunia in Gynaecological Practice: EpidemiologyDaniel ZarateNoch keine Bewertungen
- Why Does Sex Feel Good For Males and FemalesDokument17 SeitenWhy Does Sex Feel Good For Males and Femalessiesmann0% (1)
- DickDokument6 SeitenDickNadirah Abd HamidNoch keine Bewertungen
- Casanova's Dark ArtsDokument141 SeitenCasanova's Dark ArtsMartin MarkovicNoch keine Bewertungen
- Shy BookletDokument28 SeitenShy BookletDesmond ScottNoch keine Bewertungen
- Dyspareunia Due To A General Medical ConditionDokument18 SeitenDyspareunia Due To A General Medical ConditionanisNoch keine Bewertungen
- Sexuality and Sexual Disorders: Jeremi I. Cobarde Bsn-IiiDokument8 SeitenSexuality and Sexual Disorders: Jeremi I. Cobarde Bsn-IiiNikki BrodethNoch keine Bewertungen
- 12 de Veyra 1 1Dokument5 Seiten12 de Veyra 1 1Kyla Lorena Malate AbelloNoch keine Bewertungen
- The Female Price of Male PleasureDokument13 SeitenThe Female Price of Male PleasureSusanny Martin del CNoch keine Bewertungen
- Chapter 10: Sexual and Gender Identity DisordersDokument48 SeitenChapter 10: Sexual and Gender Identity DisordersSamueNoch keine Bewertungen
- Disorders Involving Gender and Sexuality EditedDokument10 SeitenDisorders Involving Gender and Sexuality EditedMike ChavezNoch keine Bewertungen
- Unpacking The Self The Sexual Self SexDokument5 SeitenUnpacking The Self The Sexual Self SexPauline Apa-apNoch keine Bewertungen
- ThesisDokument23 SeitenThesisAnushika AgarwalNoch keine Bewertungen
- Gynecologic NursingDokument218 SeitenGynecologic Nursingblacklilha100% (1)
- Human Sexuality and Sexual DysfunctionsDokument53 SeitenHuman Sexuality and Sexual DysfunctionsVincent De AsisNoch keine Bewertungen
- The Morality of Human SexualityDokument52 SeitenThe Morality of Human SexualityPaulette OliscoNoch keine Bewertungen
- Abnormal Psychology Chapter 13Dokument84 SeitenAbnormal Psychology Chapter 13Summer LeeNoch keine Bewertungen
- Vaginal DischargeDokument1 SeiteVaginal DischargeRAHMANoch keine Bewertungen
- Sexual DysfunctionsDokument59 SeitenSexual DysfunctionsJahnvi KumarNoch keine Bewertungen
- DILATOR SET Deluxe Silicone Dilator SetDokument1 SeiteDILATOR SET Deluxe Silicone Dilator SetrizaNoch keine Bewertungen
- Female Genital Mutilation (FGM) Frequently Asked QuestionsDokument47 SeitenFemale Genital Mutilation (FGM) Frequently Asked QuestionsfdskndNoch keine Bewertungen
- Rev 4 - General Gynecology 2022Dokument28 SeitenRev 4 - General Gynecology 2022Omar MohammedNoch keine Bewertungen
- ICS Standards 2019Dokument936 SeitenICS Standards 2019Gleiciane AguiarNoch keine Bewertungen
- HX Taking Reproductive SystemDokument78 SeitenHX Taking Reproductive SystemMuskaan ZaharaNoch keine Bewertungen