Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- SOP Stroke RehabilitationDokument43 SeitenSOP Stroke RehabilitationThanty Putrantii WijayantiNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Effects of Massage Therapy On Pain Management in The Acute Care SettingDokument8 SeitenThe Effects of Massage Therapy On Pain Management in The Acute Care SettingThanty Putrantii WijayantiNoch keine Bewertungen
- Intervensi Keperawatan Pada Anak Asma Dengan Diagnosa Ketidakefektifan Bersihan Jalan NapasDokument7 SeitenIntervensi Keperawatan Pada Anak Asma Dengan Diagnosa Ketidakefektifan Bersihan Jalan NapasThanty Putrantii WijayantiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Chronic Obstructive Pulmonary DiseaseDokument9 SeitenChronic Obstructive Pulmonary DiseaseThanty Putrantii WijayantiNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
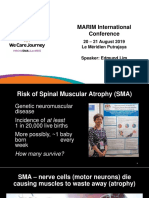
- WeCareJourney Edmund LimDokument12 SeitenWeCareJourney Edmund LimPrabhuNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- 6d52cb67c16c45b194398c6189999984Dokument196 Seiten6d52cb67c16c45b194398c6189999984SasiRekhaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Anatomy and Physiology of BloodDokument10 SeitenAnatomy and Physiology of Bloodaoi_rachelle100% (1)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Competency 3 DoneDokument2 SeitenCompetency 3 Doneapi-264474189Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Intermaxillary Relations RecordsDokument17 SeitenIntermaxillary Relations RecordsMega ShyamNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Pemeriksaan Neurologi BaruDokument45 SeitenPemeriksaan Neurologi BaruSilaturrahman IkhlasjaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Abdominal TB Causing Intestinal ObstructionDokument10 SeitenAbdominal TB Causing Intestinal ObstructionCleoanne GallegosNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- EnterotoxemiaDokument11 SeitenEnterotoxemiaabdul mananNoch keine Bewertungen
- Repair Reline & Rebase 1Dokument51 SeitenRepair Reline & Rebase 1huma100% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- NEMATODESDokument4 SeitenNEMATODESAbby VillamuchoNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Animal Tissues SummativeDokument1 SeiteAnimal Tissues SummativeLouie Jane EleccionNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDokument3 SeitenViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Encyclopedia of Feline NutritionDokument506 SeitenEncyclopedia of Feline NutritionBubu Coco100% (3)
- Rabies and Rabies-Related Lyssaviruses: ImportanceDokument10 SeitenRabies and Rabies-Related Lyssaviruses: ImportanceSophieNoch keine Bewertungen
- RatDokument2 SeitenRatAriel ChouNoch keine Bewertungen
- Applied Equine Nutrition and TrainingDokument232 SeitenApplied Equine Nutrition and TrainingAndrea Villanueva50% (2)
- Pamukkale - Turkey's Cotton CastleDokument11 SeitenPamukkale - Turkey's Cotton CastleAnasNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- SimsVIP - S Sims 4 Cheats Guide (Single Page)Dokument36 SeitenSimsVIP - S Sims 4 Cheats Guide (Single Page)Daffa Rizal100% (2)
- Venomous ArthropodsDokument24 SeitenVenomous ArthropodsYuu Ayu'k LifestarNoch keine Bewertungen
- Marinatos, MorganDokument5 SeitenMarinatos, MorganjudithNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Test Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th EditionDokument35 SeitenTest Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th Editionpledgerzea.rus7as100% (34)
- Food Borne Diseases and Its PreventionDokument181 SeitenFood Borne Diseases and Its Preventionapi-19916399Noch keine Bewertungen
- Case Presentation (Age) NG Grp. A2 FinalDokument43 SeitenCase Presentation (Age) NG Grp. A2 Finaljean therese83% (6)
- Meat Inspection GuidelineDokument43 SeitenMeat Inspection GuidelineABOHEMEED ALY0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Pemasangan Kateter UrinDokument12 SeitenPemasangan Kateter UrinYULI222100% (1)
- Primary Carcinoid Tumor of The Urinary BladderDokument5 SeitenPrimary Carcinoid Tumor of The Urinary BladdermikalraNoch keine Bewertungen
- 501 1267 1 SM PDFDokument8 Seiten501 1267 1 SM PDFyamahar1yr6Noch keine Bewertungen
- Notes On The Thorax: Anatomy RHS 241Dokument71 SeitenNotes On The Thorax: Anatomy RHS 241William JonathanNoch keine Bewertungen
- DK Dorling Kindersley - Bugs - Look CloserDokument23 SeitenDK Dorling Kindersley - Bugs - Look CloserJoshua GreenNoch keine Bewertungen
- DoYouHaveAFungalOrParasiteInfection by PaulChekDokument17 SeitenDoYouHaveAFungalOrParasiteInfection by PaulChekharmziie100% (4)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)