Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
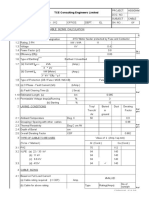
- Cable Sizing CalculationDokument72 SeitenCable Sizing CalculationHARI my songs100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Iec 60243-1-2013Dokument58 SeitenIec 60243-1-2013FernandoCrespoMon100% (1)
- Once Through: Steam GeneratorsDokument21 SeitenOnce Through: Steam GeneratorsrajrampallyNoch keine Bewertungen
- Hiley TableDokument5 SeitenHiley TableHanafiahHamzahNoch keine Bewertungen
- Chem Cheat Sheet MasterDokument6 SeitenChem Cheat Sheet MasteradamhamelehNoch keine Bewertungen
- A Report On Traffic Volume StudyDokument33 SeitenA Report On Traffic Volume StudyManoj Durairaj100% (1)
- Pavement Materials - AggregatesDokument14 SeitenPavement Materials - AggregatestombasinghNoch keine Bewertungen
- 0606 Additional Mathematics: MARK SCHEME For The May/June 2015 SeriesDokument9 Seiten0606 Additional Mathematics: MARK SCHEME For The May/June 2015 Serieswai yanNoch keine Bewertungen
- Product Bulletin N 6: Bearing Assemblies - Shaft VariationsDokument1 SeiteProduct Bulletin N 6: Bearing Assemblies - Shaft VariationsRANAIVOARIMANANANoch keine Bewertungen
- Yang Learning Face Age CVPR 2018 PaperDokument9 SeitenYang Learning Face Age CVPR 2018 Paperandr234ibateraNoch keine Bewertungen
- ASCE 7 ASD Basic Load CombosDokument1 SeiteASCE 7 ASD Basic Load CombosAamirShabbirNoch keine Bewertungen
- Auto-Tune Pid Temperature & Timer General Specifications: N L1 L2 L3Dokument4 SeitenAuto-Tune Pid Temperature & Timer General Specifications: N L1 L2 L3sharawany 20Noch keine Bewertungen
- Gps Vehicle Tracker User Manual: PrefaceDokument13 SeitenGps Vehicle Tracker User Manual: PrefaceFedericoNoch keine Bewertungen
- Integrals - Integral Calculus - Math - Khan Academy PDFDokument7 SeitenIntegrals - Integral Calculus - Math - Khan Academy PDFroberteleeroyNoch keine Bewertungen
- JSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogDokument7 SeitenJSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogMartin MurciegoNoch keine Bewertungen
- Ace Om 230Dokument3 SeitenAce Om 230michaelliu123456Noch keine Bewertungen
- Spesiikasi PerallatanDokument10 SeitenSpesiikasi PerallatanRafi RaziqNoch keine Bewertungen
- LCS21 - 35 - Polar PlotsDokument14 SeitenLCS21 - 35 - Polar Plotsgosek16375Noch keine Bewertungen
- Chapter 1: Coding Decoding: Important Note: It Is Good To Avoid Pre-Defined Coding Rule To Write A Coded MessageDokument7 SeitenChapter 1: Coding Decoding: Important Note: It Is Good To Avoid Pre-Defined Coding Rule To Write A Coded MessageUmamNoch keine Bewertungen
- IIM Nagpur Test 1 Version 1 2016Dokument6 SeitenIIM Nagpur Test 1 Version 1 2016Saksham GoyalNoch keine Bewertungen
- Tlsiw - Class X - Project Details - 2023-24Dokument2 SeitenTlsiw - Class X - Project Details - 2023-24how toNoch keine Bewertungen
- Gantt ChartDokument4 SeitenGantt ChartSyed FaridNoch keine Bewertungen
- Teaching and Learning Plan (TLP) : S. P. Mandali'S Prin L. N. Welingkar Institute of Management Development & ResearchDokument6 SeitenTeaching and Learning Plan (TLP) : S. P. Mandali'S Prin L. N. Welingkar Institute of Management Development & ResearchBhagath VarenyaNoch keine Bewertungen
- 20CB PDFDokument59 Seiten20CB PDFChidiebere Samuel OkogwuNoch keine Bewertungen
- HST TrainingDokument11 SeitenHST TrainingRamesh BabuNoch keine Bewertungen
- 23AE23 DS enDokument4 Seiten23AE23 DS enBhageerathi SahuNoch keine Bewertungen
- 1 s2.0 0304386X9190055Q MainDokument32 Seiten1 s2.0 0304386X9190055Q MainJordan Ulloa Bello100% (1)
- Spelling RulesDokument5 SeitenSpelling RulesvijthorNoch keine Bewertungen
- 15Dokument20 Seiten15Allen Rey YeclaNoch keine Bewertungen
- Rekonfigurasi Jaringan Distribusi Radial Untuk Mengurangi Rugi Daya Pada Penyulang Jatirejo Rayon Mojoagung Menggunakan Metode BinaryDokument4 SeitenRekonfigurasi Jaringan Distribusi Radial Untuk Mengurangi Rugi Daya Pada Penyulang Jatirejo Rayon Mojoagung Menggunakan Metode BinaryNurindra CahyantaNoch keine Bewertungen