Das könnte Ihnen auch gefallen
- Nursing Care for High-Risk Labor and DeliveryDokument170 SeitenNursing Care for High-Risk Labor and DeliveryLongyapon Sheena Stephanie100% (2)
- 3 Problems With The Passenger and Powers of LaborDokument105 Seiten3 Problems With The Passenger and Powers of LaborRaquel M. MendozaNoch keine Bewertungen
- Labor & DeliveryDokument14 SeitenLabor & DeliveryNiña Eleana FranciscoNoch keine Bewertungen
- Maternal and Child Nursing Module 1: Obstetric Nursing OverviewDokument18 SeitenMaternal and Child Nursing Module 1: Obstetric Nursing Overviewjanina myka100% (1)
- Placenta and Placental ProblemsDokument13 SeitenPlacenta and Placental ProblemsLuvita Ronteltap100% (1)
- Management of Normal Labor and DeliveryDokument40 SeitenManagement of Normal Labor and Deliveryrendyprimananda840Noch keine Bewertungen
- Tocolytic Treatment in PregnancyDokument21 SeitenTocolytic Treatment in PregnancyxxdrivexxNoch keine Bewertungen
- Care of the NewbornDokument6 SeitenCare of the NewbornJankie Obina Alcaba100% (1)
- Problems With Passenger and PowerDokument6 SeitenProblems With Passenger and PowerhoohooNoch keine Bewertungen
- The High Risk Prenatal ClientDokument46 SeitenThe High Risk Prenatal ClientPaul Albert Agunod100% (2)
- OB RNSG 2208 Mid-term OutlineDokument23 SeitenOB RNSG 2208 Mid-term OutlineAnnissaLarnardNoch keine Bewertungen
- High Risk PregnancyDokument2 SeitenHigh Risk PregnancyCaren ReyesNoch keine Bewertungen
- NCM 102 Power and PsycheDokument13 SeitenNCM 102 Power and Psychelarissedeleon100% (1)
- NCM 102 Course OutlineDokument13 SeitenNCM 102 Course OutlineMichael Gustilo100% (1)
- High - Risk PregnancyDokument110 SeitenHigh - Risk PregnancyAndre DityaNoch keine Bewertungen
- Step To Follow Intrapartal CareDokument3 SeitenStep To Follow Intrapartal CareyabaeveNoch keine Bewertungen
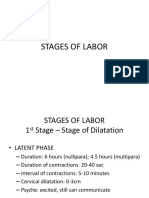
- Stages of LaborDokument14 SeitenStages of LaborKimberly CostalesNoch keine Bewertungen
- Care of High Risk Pregnant MothersDokument10 SeitenCare of High Risk Pregnant MothersJaimie BanaagNoch keine Bewertungen
- NonStress TestDokument2 SeitenNonStress TestRama_ichiNoch keine Bewertungen
- Sample of MMDSTDokument32 SeitenSample of MMDSTBeverly PatriarcaNoch keine Bewertungen
- Nursing Care for Women with Intrapartum ComplicationsDokument70 SeitenNursing Care for Women with Intrapartum ComplicationsRose AnnNoch keine Bewertungen
- Theories of Labor OnsetDokument4 SeitenTheories of Labor OnsetCzarina PorciunculaNoch keine Bewertungen
- MCH BulletsDokument13 SeitenMCH BulletsPatziedawn GonzalvoNoch keine Bewertungen
- Obsteric EmergenciesDokument48 SeitenObsteric EmergenciesNurul AshikinNoch keine Bewertungen
- Nursing Care of A Family When A Child Has A Neurologic DisorderDokument8 SeitenNursing Care of A Family When A Child Has A Neurologic DisorderBern NerquitNoch keine Bewertungen
- Complications in PregnancyDokument81 SeitenComplications in PregnancyTia TahniaNoch keine Bewertungen
- Apgar ScoreDokument2 SeitenApgar Scorejulialeo100% (3)
- Ob 3 SetsDokument6 SeitenOb 3 Setshananchloe25100% (1)
- NCM 102Dokument8 SeitenNCM 102lemuel_que100% (2)
- Immaculate Conception College-Albay Daraga, Albay NCM 102Dokument2 SeitenImmaculate Conception College-Albay Daraga, Albay NCM 102Paul Jhon Vergara100% (3)
- High Risk PregnancyDokument14 SeitenHigh Risk PregnancyJezrael PueblosNoch keine Bewertungen
- Placental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Dokument3 SeitenPlacental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Mary AgorillaNoch keine Bewertungen
- MCN Lab - M7 - INTRAPARTUM CARE 2020-2021Dokument28 SeitenMCN Lab - M7 - INTRAPARTUM CARE 2020-2021Kristine Kim100% (1)
- 1 N-109 MCN 2 LEC Syllabus (2 S, AY 19-20) REVISED PDFDokument7 Seiten1 N-109 MCN 2 LEC Syllabus (2 S, AY 19-20) REVISED PDFCayla Mae CarlosNoch keine Bewertungen
- Bubblehe PDFDokument3 SeitenBubblehe PDFHenny Kim100% (1)
- Placental AbnormalitiesDokument42 SeitenPlacental AbnormalitiesTee VillanuevaNoch keine Bewertungen
- Prolonged LaborDokument32 SeitenProlonged Labormaezu50% (2)
- A. Dystocia: Problems With PowerDokument48 SeitenA. Dystocia: Problems With PowerPauline GarciaNoch keine Bewertungen
- Mechanisms of LaborDokument16 SeitenMechanisms of LaborRyan Robert V. Ventolero100% (1)
- Prenatal Management (Part 4)Dokument17 SeitenPrenatal Management (Part 4)Austine James Sabenicio PantiloNoch keine Bewertungen
- Female Reproductive System and Childbirth ProcessesDokument64 SeitenFemale Reproductive System and Childbirth ProcessesIvory SantiagoNoch keine Bewertungen
- Stages of Labor and DeliveryDokument7 SeitenStages of Labor and DeliveryAijem Ryan86% (7)
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYDokument5 SeitenUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)
- Immediate Newborn Care-DOH 2010Dokument2 SeitenImmediate Newborn Care-DOH 2010fegerilene100% (2)
- Clinical Guidelines on Intrapartum and Postpartum CareDokument52 SeitenClinical Guidelines on Intrapartum and Postpartum CareAngela SaldajenoNoch keine Bewertungen
- HO 4 Essential Intrapartum Care 6may2013Dokument12 SeitenHO 4 Essential Intrapartum Care 6may2013Maedine Urbano-Briones100% (1)
- NSDDokument44 SeitenNSDabyssodeep100% (1)
- C-Section Procedure GuideDokument4 SeitenC-Section Procedure GuideKeanu ArcillaNoch keine Bewertungen
- OB Definition of TermsDokument9 SeitenOB Definition of TermsWarrenSandovalNoch keine Bewertungen
- High Risk Prenatal ClientDokument10 SeitenHigh Risk Prenatal ClientAudreySalvador100% (1)
- Cord CoilDokument2 SeitenCord CoilAlphine DalgoNoch keine Bewertungen
- Normal Labor and DeliveryDokument45 SeitenNormal Labor and DeliveryZari NovelaNoch keine Bewertungen
- Post Partum Depression Final Presentation 2Dokument7 SeitenPost Partum Depression Final Presentation 2api-506871797100% (1)
- Placenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaDokument72 SeitenPlacenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaEsa SthaNoch keine Bewertungen
- OBG Nursing Dept ReportDokument14 SeitenOBG Nursing Dept ReportAnjali Rahul AjmeriNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Fetal MalpresentationDokument83 SeitenFetal MalpresentationArianJubaneNoch keine Bewertungen
- Fetal MalpresentationDokument13 SeitenFetal MalpresentationJhing Rodriguez Borjal75% (4)
- Prepared by Marjorie Galicia Romano Clinical InstructorDokument106 SeitenPrepared by Marjorie Galicia Romano Clinical InstructorMarjorie Galicia Romano-AndalisNoch keine Bewertungen
- Intrapartal ComplicationsDokument5 SeitenIntrapartal ComplicationsJeremiah JustoNoch keine Bewertungen
- Nutrition in PregnancyDokument60 SeitenNutrition in PregnancylarissedeleonNoch keine Bewertungen
- Care of Patients With Neurological DisordersDokument82 SeitenCare of Patients With Neurological Disorderslarissedeleon100% (1)
- MNT in Diabetes and Related Disorders and StrategiesDokument122 SeitenMNT in Diabetes and Related Disorders and StrategieslarissedeleonNoch keine Bewertungen
- NCM 102 - High Risk NewbornDokument4 SeitenNCM 102 - High Risk NewbornlarissedeleonNoch keine Bewertungen
- NCM 102 Puerperal InfectionDokument8 SeitenNCM 102 Puerperal InfectionlarissedeleonNoch keine Bewertungen
- NCM 102 Post Partal Complications HemorrhageDokument10 SeitenNCM 102 Post Partal Complications HemorrhagelarissedeleonNoch keine Bewertungen
- Pre Gestational ConditionsDokument17 SeitenPre Gestational Conditionslarissedeleon100% (2)
- NCM 102 Power and PsycheDokument13 SeitenNCM 102 Power and Psychelarissedeleon100% (1)
- NCM 102 - Anesthesia and AnalgesiaDokument3 SeitenNCM 102 - Anesthesia and AnalgesialarissedeleonNoch keine Bewertungen
- Pathophysiology FinalDokument2 SeitenPathophysiology FinallarissedeleonNoch keine Bewertungen
- CVD Infarct-HpniiDokument3 SeitenCVD Infarct-HpniilarissedeleonNoch keine Bewertungen
- COMDISEASEDokument39 SeitenCOMDISEASElarissedeleonNoch keine Bewertungen
- CA 2 LMR Handout 2s1314Dokument8 SeitenCA 2 LMR Handout 2s1314larissedeleonNoch keine Bewertungen
- Acute TonsillopharyngitisDokument13 SeitenAcute TonsillopharyngitislarissedeleonNoch keine Bewertungen
- Myocardial InfarctionDokument4 SeitenMyocardial InfarctionlarissedeleonNoch keine Bewertungen
- PRC Cases FormDokument4 SeitenPRC Cases FormlarissedeleonNoch keine Bewertungen
- Ca1 - Coronary Artery Bypass GraftDokument5 SeitenCa1 - Coronary Artery Bypass GraftlarissedeleonNoch keine Bewertungen
- NursesDokument2 SeitenNursesDhingskie100% (5)
- Ketoacidosis, DysrhythmiasDokument39 SeitenKetoacidosis, DysrhythmiaslarissedeleonNoch keine Bewertungen
- Cervical Cancer 2.0Dokument9 SeitenCervical Cancer 2.0larissedeleonNoch keine Bewertungen
- Chapters15 20&24Dokument64 SeitenChapters15 20&24larissedeleonNoch keine Bewertungen
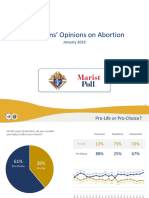
- 2023 Kofc Marist Poll PresentationDokument14 Seiten2023 Kofc Marist Poll PresentationVeronica SilveriNoch keine Bewertungen
- Journal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresDokument6 SeitenJournal Critiquing Article Reviewed:: Submitted To: Prof. Cynthia A. Umila, RN, MAN Submitted By: Yvette Claire L. BorresYVETTE CLAIRE BORRESNoch keine Bewertungen
- Er DR Ward ScriptDokument3 SeitenEr DR Ward ScriptChristine Mae MacatangayNoch keine Bewertungen
- Concepts of Growth and Development: The Capacity and Skill of A Person To Function "The Behavioral Aspect of Growth"Dokument75 SeitenConcepts of Growth and Development: The Capacity and Skill of A Person To Function "The Behavioral Aspect of Growth"Crizza PunzalNoch keine Bewertungen
- Board Question Paper - March 2023 - For Reprint Update - 641b040f4992cDokument4 SeitenBoard Question Paper - March 2023 - For Reprint Update - 641b040f4992cSushan BhagatNoch keine Bewertungen
- Postpartum Health TeachingDokument8 SeitenPostpartum Health TeachingMsOrange96% (24)
- Nausea and Vomiting of Pregnancy and Hyperemesis GravidarumDokument27 SeitenNausea and Vomiting of Pregnancy and Hyperemesis GravidarumxxdrivexxNoch keine Bewertungen
- Lesson 3 - PregnancyDokument4 SeitenLesson 3 - PregnancyA CNoch keine Bewertungen
- Physical Therapy For BeginnersDokument4 SeitenPhysical Therapy For BeginnersBogart MacatangayNoch keine Bewertungen
- Puerperium Q ADokument2 SeitenPuerperium Q AMae Rose Charlene MendozaNoch keine Bewertungen
- (2019) Fetal Movement and Stillbirth EducationDokument9 Seiten(2019) Fetal Movement and Stillbirth EducationaninditaNoch keine Bewertungen
- Case Presentation: Daguio / Dianalan / Ebrahim / EddingDokument29 SeitenCase Presentation: Daguio / Dianalan / Ebrahim / EddingnsdnNoch keine Bewertungen
- Lecture 3 Associated Risk FactorsDokument55 SeitenLecture 3 Associated Risk FactorsTHANISHTA KUMARNoch keine Bewertungen
- Clinics in Mother & Child Health: Pathophysiology of EclampsiaDokument2 SeitenClinics in Mother & Child Health: Pathophysiology of EclampsiaVetta FegitalaskyNoch keine Bewertungen
- 2023 - Article - 5356Dokument9 Seiten2023 - Article - 5356indahrizkygNoch keine Bewertungen
- Fatigue and Back Pain NCP PresentationDokument18 SeitenFatigue and Back Pain NCP PresentationTine Guibao100% (1)
- Drugs Used IN Pregnancy, Labour, Puerperium & NewbornDokument42 SeitenDrugs Used IN Pregnancy, Labour, Puerperium & NewbornSanjay Kumar SanjuNoch keine Bewertungen
- The Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)Dokument284 SeitenThe Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)AndreaAlexandraNoch keine Bewertungen
- Ectopic Pregnancy: Deomicah D. SolanoDokument42 SeitenEctopic Pregnancy: Deomicah D. SolanoJann ericka JaoNoch keine Bewertungen
- Fundamentals of ReproductionDokument4 SeitenFundamentals of ReproductionHalo Ini JeskryNoch keine Bewertungen
- BMHP Untuk Rekapan 2019-1Dokument10 SeitenBMHP Untuk Rekapan 2019-1memyu mahmudahNoch keine Bewertungen
- Argumentative Essay About AbortionDokument2 SeitenArgumentative Essay About AbortionJewel TanNoch keine Bewertungen
- Im Grave's DiseaseDokument28 SeitenIm Grave's DiseaseHidvardNoch keine Bewertungen
- Maternal-Fetal Circadian Communication During PregnancyDokument9 SeitenMaternal-Fetal Circadian Communication During PregnancyLeslie AcevesNoch keine Bewertungen
- Yumbe District Advocacy Strategy 2020-2030Dokument17 SeitenYumbe District Advocacy Strategy 2020-2030yumbengo forumNoch keine Bewertungen
- Cephalo Pelvic Disproportion (CPD) & Contracted PelvisDokument45 SeitenCephalo Pelvic Disproportion (CPD) & Contracted Pelvisbinipsamuel250% (1)
- STAR HEALTH INSURANCE COVER AT A GLANCEDokument21 SeitenSTAR HEALTH INSURANCE COVER AT A GLANCEMy OrthotreeNoch keine Bewertungen
- Recurrent Pregnancy LossDokument19 SeitenRecurrent Pregnancy LossSean NamNoch keine Bewertungen
- Powerful Antiviral Herbs - Free-SampleDokument30 SeitenPowerful Antiviral Herbs - Free-SampleRJKNoch keine Bewertungen
- Bioethics Offers A MultiDokument5 SeitenBioethics Offers A MultiGlaiza Mae CruzNoch keine Bewertungen