Das könnte Ihnen auch gefallen
- Neurosurgey MCQ Collection Part IDokument35 SeitenNeurosurgey MCQ Collection Part IMohammed Ali Aldhahir88% (8)
- Neurosurgery Final Exam MCQsDokument5 SeitenNeurosurgery Final Exam MCQsIbrahem Y. Najjar100% (1)
- 39 MCQ's in NeurosurgeryDokument26 Seiten39 MCQ's in NeurosurgeryAhmed Hamid Ibrahim100% (4)
- Cranial Osteomyelitis Diagnosis and Treatment OptionsDokument5 SeitenCranial Osteomyelitis Diagnosis and Treatment OptionsRajanish Kumar50% (2)
- Neuro SurgeryDokument14 SeitenNeuro Surgeryapi-3840195100% (4)
- Neurosurgery Review (PDF) (UnitedVRG) PDFDokument377 SeitenNeurosurgery Review (PDF) (UnitedVRG) PDFHo Hoang Vu80% (5)
- Colen Flash-Review Neurosurgery THIRD EDITIONDokument41 SeitenColen Flash-Review Neurosurgery THIRD EDITIONDr. Chaim B. Colen100% (3)
- Neurosurgery Question Bank TopicsDokument2 SeitenNeurosurgery Question Bank TopicsYoussry Jaranilla50% (4)
- Tanta Neuro MCQDokument9 SeitenTanta Neuro MCQBadr Diham100% (1)
- NeurosurgeryDokument38 SeitenNeurosurgeryakufahaba100% (2)
- Neurosurgery Review MCQDokument8 SeitenNeurosurgery Review MCQSyed Ali Haider100% (1)
- Neurosurgery, 1000 MCQs - بحث GoogleDokument2 SeitenNeurosurgery, 1000 MCQs - بحث Googleريماالعلي33% (3)
- MCQ NeurologyDokument18 SeitenMCQ NeurologySAlemsa0% (1)
- Neurosurgery Final Exam QuestionsDokument6 SeitenNeurosurgery Final Exam QuestionsMAMA LALANoch keine Bewertungen
- Neurology MCQDokument6 SeitenNeurology MCQMuhammad Qasum43% (7)
- NerosurgeryDokument34 SeitenNerosurgeryapi-19502000100% (1)
- MCQs NeuroDokument2 SeitenMCQs NeuroBagadi Suneel100% (2)
- Neurosurgery Quiz Question Answers (Question Bank)Dokument4 SeitenNeurosurgery Quiz Question Answers (Question Bank)İbrahim Erkutlu33% (3)
- Neuro MCQDokument4 SeitenNeuro MCQLim EricNoch keine Bewertungen
- UNIT-5 Pharmacology of NeurosurgeryDokument12 SeitenUNIT-5 Pharmacology of NeurosurgeryFaizan Mazhar100% (1)
- Neuro MCQDokument15 SeitenNeuro MCQSushanta BhanjaNoch keine Bewertungen
- Copia de 1000 Preguntas de Autoevaluacion PDFDokument658 SeitenCopia de 1000 Preguntas de Autoevaluacion PDFAnonymous FUrdgw50% (2)
- Neurosurgery Congenital Anomalies: Types & DefinitionsDokument41 SeitenNeurosurgery Congenital Anomalies: Types & DefinitionsMAYNoch keine Bewertungen
- Fracp Past Papers - NeurologyDokument21 SeitenFracp Past Papers - NeurologyLakshya J BasumataryNoch keine Bewertungen
- 2011-2012 Group 6Dokument5 Seiten2011-2012 Group 6Law YouNoch keine Bewertungen
- Neurology MCQDokument5 SeitenNeurology MCQRaghu Nadh0% (1)
- I MCQs Neuro.Dokument4 SeitenI MCQs Neuro.Mhmd Iraky100% (1)
- Final-Exam Neurosurgery - 2-VersionDokument6 SeitenFinal-Exam Neurosurgery - 2-VersionMAMA LALANoch keine Bewertungen
- Clinical Neurosurgical Vignettes For The Oral Board and Recertification Examinations First 2 Chapters PDFDokument27 SeitenClinical Neurosurgical Vignettes For The Oral Board and Recertification Examinations First 2 Chapters PDFece142100% (2)
- MCQ of NeurologyDokument45 SeitenMCQ of Neurologyeffe26100% (6)
- III. Mcqs NeuroDokument19 SeitenIII. Mcqs NeuroMhmd Iraky100% (1)
- Neurotrauma in Multiple-Choice Questions (Samer S. Hoz, Iype Cherian, Ali A. Dolachee Etc.) (Z-Library)Dokument187 SeitenNeurotrauma in Multiple-Choice Questions (Samer S. Hoz, Iype Cherian, Ali A. Dolachee Etc.) (Z-Library)Jéssica AméricoNoch keine Bewertungen
- Neurology MCQDokument3 SeitenNeurology MCQNyle GreyNoch keine Bewertungen
- MCQs TBIDokument9 SeitenMCQs TBIAkbar Ali100% (3)
- IV. Mcqs NeuroDokument7 SeitenIV. Mcqs NeuroMhmd IrakyNoch keine Bewertungen
- Teaching MCQ-Neurology BasicsDokument17 SeitenTeaching MCQ-Neurology Basicslonsilord17Noch keine Bewertungen
- 5-Neuro MCQs Final UnsolvedDokument29 Seiten5-Neuro MCQs Final UnsolvedOsman Somi0% (2)
- General Practitioner - Neurology MCQsDokument20 SeitenGeneral Practitioner - Neurology MCQsAsif Newaz100% (3)
- II. MCQs NeuroDokument13 SeitenII. MCQs NeuroMhmd Iraky100% (2)
- Cerebrovascular Disease MCQDokument25 SeitenCerebrovascular Disease MCQDr. Kishore Kumar Ubrangala85% (13)
- Risk Factors and Causes of StrokeDokument19 SeitenRisk Factors and Causes of StrokeAsif Newaz100% (2)
- GEMP IV Orthopaedics OSCE 2010Dokument39 SeitenGEMP IV Orthopaedics OSCE 2010Lana Loco50% (2)
- Neurology revision-2015: Benztropine side effects & status epilepticus treatmentsDokument99 SeitenNeurology revision-2015: Benztropine side effects & status epilepticus treatmentsPaz Vida100% (7)
- Undergraduate Neurosurgery Lecture NotesDokument124 SeitenUndergraduate Neurosurgery Lecture NotesLuquiitas LasernaNoch keine Bewertungen
- Arab Board Final 2018 - 2Dokument12 SeitenArab Board Final 2018 - 2lonsilord17Noch keine Bewertungen
- NEUROLOGY REVIEWDokument32 SeitenNEUROLOGY REVIEWNeha GoelNoch keine Bewertungen
- Neurological MCQDokument4 SeitenNeurological MCQAnonymous hF5zAdvwCC100% (1)
- Comprehensive Neurology Board Review-THIRD EDITIONDokument44 SeitenComprehensive Neurology Board Review-THIRD EDITIONDr. Chaim B. Colen50% (4)
- Trauma MCQ DiDokument13 SeitenTrauma MCQ DiJohn M. HemsworthNoch keine Bewertungen
- Neurosurgery: UnprotectedDokument39 SeitenNeurosurgery: UnprotectedMaulana Taufik100% (2)
- Neurology: Self-Assessment for MRCP(UK) Neurology SCEVon EverandNeurology: Self-Assessment for MRCP(UK) Neurology SCEBewertung: 5 von 5 Sternen5/5 (1)
- Multiple Choice Questions in Paediatric SurgeryVon EverandMultiple Choice Questions in Paediatric SurgeryBewertung: 1 von 5 Sternen1/5 (1)
- Neurology Multiple Choice Questions With Explanations: Volume IIIVon EverandNeurology Multiple Choice Questions With Explanations: Volume IIIBewertung: 4.5 von 5 Sternen4.5/5 (6)
- Neurology Multiple Choice Questions With Explanations: Volume IVon EverandNeurology Multiple Choice Questions With Explanations: Volume IBewertung: 4 von 5 Sternen4/5 (7)
- Multiple Choice Questions in Ophthalmic and NeuroanatomyVon EverandMultiple Choice Questions in Ophthalmic and NeuroanatomyNoch keine Bewertungen
- Neurology Multiple Choice Questions With Explanations: Volume IIVon EverandNeurology Multiple Choice Questions With Explanations: Volume IIBewertung: 5 von 5 Sternen5/5 (2)
- Physiology and Pathology of Physical and Psychological StressDokument60 SeitenPhysiology and Pathology of Physical and Psychological StressBrunoNoch keine Bewertungen
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDokument40 SeitenProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoNoch keine Bewertungen
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDokument25 SeitenDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoNoch keine Bewertungen
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDokument11 SeitenMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoNoch keine Bewertungen
- TAEI NTRI WorkshopDokument16 SeitenTAEI NTRI WorkshopBrunoNoch keine Bewertungen
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDokument42 SeitenProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoNoch keine Bewertungen
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDokument32 SeitenDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDokument36 SeitenDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- Ms Ellaine Boo Role of Trauma NursingDokument35 SeitenMs Ellaine Boo Role of Trauma NursingBrunoNoch keine Bewertungen
- DR - Joseph Mathew: Trauma Units and Team WorkDokument39 SeitenDR - Joseph Mathew: Trauma Units and Team WorkBrunoNoch keine Bewertungen
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDokument16 SeitenHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoNoch keine Bewertungen
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDokument37 SeitenProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoNoch keine Bewertungen
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDokument25 SeitenMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDokument36 SeitenProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoNoch keine Bewertungen
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDokument73 SeitenDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoNoch keine Bewertungen
- TN Gazette 47 of 2013 Part VI Section 4Dokument84 SeitenTN Gazette 47 of 2013 Part VI Section 4BrunoNoch keine Bewertungen
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaDokument77 SeitenProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
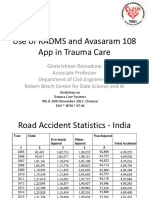
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDokument21 SeitenProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoNoch keine Bewertungen
- Doctors' Role in Tackling Organ TradeDokument70 SeitenDoctors' Role in Tackling Organ TradeBrunoNoch keine Bewertungen
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDokument46 SeitenProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoNoch keine Bewertungen
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDokument26 SeitenIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoNoch keine Bewertungen
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDokument29 SeitenDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoNoch keine Bewertungen
- DR - Darez Ahamed Vision For Tamil NaduDokument6 SeitenDR - Darez Ahamed Vision For Tamil NaduBrunoNoch keine Bewertungen
- Neurosurgeon For A Social CauseDokument55 SeitenNeurosurgeon For A Social CauseBrunoNoch keine Bewertungen
- How Tamil Nadu Eradicated Organ SaleDokument108 SeitenHow Tamil Nadu Eradicated Organ SaleBrunoNoch keine Bewertungen
- AR Rahman PDFDokument405 SeitenAR Rahman PDFPitchai BalaNoch keine Bewertungen
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDokument52 SeitenWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoNoch keine Bewertungen
- HMIS - Health Management Information System - Government of Tamil NaduDokument12 SeitenHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- NEET PG 2013 Rank List of Eligible CandidatesDokument256 SeitenNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- Traumatic Brain Injury (TBI) - Definition, Epidemiology, PathophysiologyDokument10 SeitenTraumatic Brain Injury (TBI) - Definition, Epidemiology, Pathophysiologypetremure2147Noch keine Bewertungen
- Intracranial HypertensionDokument28 SeitenIntracranial HypertensionHussein TarhiniNoch keine Bewertungen
- DocxDokument53 SeitenDocxkuro hanabusaNoch keine Bewertungen
- Head injuries require urgent careDokument7 SeitenHead injuries require urgent careSariiNoch keine Bewertungen
- Brain Herniation: April 2020Dokument13 SeitenBrain Herniation: April 2020Athira PSNoch keine Bewertungen
- Quiz With Answer and RationaleDokument4 SeitenQuiz With Answer and Rationaleann aquinoNoch keine Bewertungen
- Nursing considerations for clients on loop diuretics and beta blockersDokument59 SeitenNursing considerations for clients on loop diuretics and beta blockersGil Raphael GanibanNoch keine Bewertungen
- Procedural Report CraniectomyDokument3 SeitenProcedural Report CraniectomyAubrey UniqueNoch keine Bewertungen
- Headache When To WorryDokument9 SeitenHeadache When To Worryezra_putriNoch keine Bewertungen
- Guide to Evaluating and Diagnosing Common Headache DisordersDokument54 SeitenGuide to Evaluating and Diagnosing Common Headache DisorderssaharuiNoch keine Bewertungen
- The Medical Disability Advisor: Workplace Guidelines For Disability DurationDokument4 SeitenThe Medical Disability Advisor: Workplace Guidelines For Disability DurationnsatriotomoNoch keine Bewertungen
- Case Study ExampleDokument46 SeitenCase Study ExampleDerick PaguiriganNoch keine Bewertungen
- DR - Roezwir SP.SDokument76 SeitenDR - Roezwir SP.SSyifaAsriFauziahNoch keine Bewertungen
- Severity Assessment and Scoring For Neurosurgical Models in RodentsDokument11 SeitenSeverity Assessment and Scoring For Neurosurgical Models in RodentsKazhi SujudNoch keine Bewertungen
- Use A "GHOST-CAP" in Acute Brain Injury: Editorial Open AccessDokument3 SeitenUse A "GHOST-CAP" in Acute Brain Injury: Editorial Open Accessdiana ramirezNoch keine Bewertungen
- Meningitis PPT 2.0Dokument15 SeitenMeningitis PPT 2.0Francis Adrian100% (1)
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sDokument4 Seiten"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersNoch keine Bewertungen
- Brain Injury: Closed (Blunt) Brain Injury Occurs When The Head Accelerates and ThenDokument7 SeitenBrain Injury: Closed (Blunt) Brain Injury Occurs When The Head Accelerates and Thencute_tineeNoch keine Bewertungen
- College of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisDokument9 SeitenCollege of Nursing Berhampur: Subject-Medical Surgical Nursing Topic-MeningitisAmlan jyoti thanapati100% (1)
- Neurology Past Years Before EhsanDokument345 SeitenNeurology Past Years Before EhsanMohammad AlrefaiNoch keine Bewertungen
- Pathophysiology HeadinjuryDokument1 SeitePathophysiology HeadinjuryK.b. Dequiña100% (1)
- Approach To Comatose Child: DR G.VenkateshDokument83 SeitenApproach To Comatose Child: DR G.VenkateshG VenkateshNoch keine Bewertungen
- Anaesthesia For NeurosurgeryDokument4 SeitenAnaesthesia For NeurosurgeryjcaegNoch keine Bewertungen
- Wilderness MedicineDokument109 SeitenWilderness Medicinemichaearth100% (2)
- Hesi ReviewDokument59 SeitenHesi ReviewKrista Howe100% (3)
- Tema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónDokument17 SeitenTema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónaniadNoch keine Bewertungen
- ICU/CCU Only Competencies and Johns Hopkins MHA ICU ProjectDokument107 SeitenICU/CCU Only Competencies and Johns Hopkins MHA ICU Projecthery100% (2)
- Differential Diagnosis of Papilledema - UpToDateDokument28 SeitenDifferential Diagnosis of Papilledema - UpToDateDaniel PadillaNoch keine Bewertungen
- Pathophysiology of Brain TumorsDokument2 SeitenPathophysiology of Brain TumorsNavjot Brar92% (13)
- Increased Intracranial PressureDokument4 SeitenIncreased Intracranial PressureratihNoch keine Bewertungen