Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Renr Study GuideDokument57 SeitenRenr Study GuideJerilee SoCute Watts92% (12)
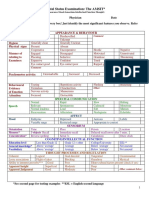
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDokument2 SeitenMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Current Trends in Sterilisation of Operation TheatresDokument7 SeitenCurrent Trends in Sterilisation of Operation Theatrestummalapalli venkateswara raoNoch keine Bewertungen
- Artificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDDokument34 SeitenArtificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Screening For MRSA by Dr.T.V.Rao MDDokument30 SeitenScreening For MRSA by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDokument100 SeitenInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- HOSPITAL ANTIBIOGRAMS Principles Interpretation and DocumentationDokument55 SeitenHOSPITAL ANTIBIOGRAMS Principles Interpretation and Documentationtummalapalli venkateswara raoNoch keine Bewertungen
- Fall Out of Neet On Medical EdcuationDokument2 SeitenFall Out of Neet On Medical Edcuationtummalapalli venkateswara raoNoch keine Bewertungen
- MEDICAL ETHICS IN RESEARCH PROPOSALS (Indian Contest)Dokument62 SeitenMEDICAL ETHICS IN RESEARCH PROPOSALS (Indian Contest)tummalapalli venkateswara raoNoch keine Bewertungen
- Surgical Operation Theater StandardsDokument31 SeitenSurgical Operation Theater Standardstummalapalli venkateswara raoNoch keine Bewertungen
- Need For Clinical Microbiologists by Dr.T.V.Rao MDDokument2 SeitenNeed For Clinical Microbiologists by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Our Vison To Future On Diagnostic Microbiology by Dr.T.V.Rao MDDokument5 SeitenOur Vison To Future On Diagnostic Microbiology by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- MDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDDokument2 SeitenMDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- JOURNAL CLUB in Medicine Preparation and Presentation Dr.T.V.Rao MDDokument36 SeitenJOURNAL CLUB in Medicine Preparation and Presentation Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Streaking Culture Plates in Bacteriology by Dr.T.V.Rao MDDokument33 SeitenStreaking Culture Plates in Bacteriology by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- School Hygiene by Dr.T.V.Rao MDDokument32 SeitenSchool Hygiene by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Who Is Killing Modern Medicine in IndiaDokument3 SeitenWho Is Killing Modern Medicine in Indiatummalapalli venkateswara raoNoch keine Bewertungen
- Hand Hygiene and Prevention of Infection inDokument22 SeitenHand Hygiene and Prevention of Infection intummalapalli venkateswara raoNoch keine Bewertungen
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDokument33 SeitenMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDokument2 SeitenGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDokument28 SeitenElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- 10 Options To Control Hospital Infections by Dr.T.V.Rao MDDokument17 Seiten10 Options To Control Hospital Infections by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- School Hygiene Preventing InfectionsDokument19 SeitenSchool Hygiene Preventing Infectionstummalapalli venkateswara raoNoch keine Bewertungen
- INTERPRETATION OF ANTIBIOGRAMS Trends of Change by Dr.T.V.Rao MDDokument62 SeitenINTERPRETATION OF ANTIBIOGRAMS Trends of Change by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Health Care Associated Infections Creating Drug Resistance AtlasDokument46 SeitenHealth Care Associated Infections Creating Drug Resistance Atlastummalapalli venkateswara raoNoch keine Bewertungen
- Infection Control in Burns PatietnsDokument41 SeitenInfection Control in Burns Patietnstummalapalli venkateswara raoNoch keine Bewertungen
- INFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDDokument25 SeitenINFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- MALDI-ToF in Clinical MicrobiologyDokument39 SeitenMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- MDR-TB An Update by Dr.T.V.Rao MDDokument43 SeitenMDR-TB An Update by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDokument61 SeitenHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoNoch keine Bewertungen
- World TB Day 2016Dokument33 SeitenWorld TB Day 2016tummalapalli venkateswara raoNoch keine Bewertungen
- Oral Cancer BDADokument36 SeitenOral Cancer BDAJesús De Santos AlbaNoch keine Bewertungen
- Agen HematinikDokument77 SeitenAgen HematinikErinaGeraldiNoch keine Bewertungen
- Maternal Pulse Pressure and The Risk of Postepidural ComplicationsDokument11 SeitenMaternal Pulse Pressure and The Risk of Postepidural ComplicationsRiany Jade SabrinaNoch keine Bewertungen
- CFS - Denigration by DesignDokument246 SeitenCFS - Denigration by Designfatima110Noch keine Bewertungen
- Understanding Laryngopharyngeal Reflux DiseaseDokument30 SeitenUnderstanding Laryngopharyngeal Reflux Diseaseamitkulkarni83100% (1)
- RENR Review Utech 8Dokument34 SeitenRENR Review Utech 8natalieshirley100% (3)
- Ross Case Book 2016Dokument305 SeitenRoss Case Book 2016S86% (7)
- Bionator: The Father of Functional OrthodonticsDokument307 SeitenBionator: The Father of Functional OrthodonticsApurava Singh100% (3)
- Avi Kremer Case AnalysisDokument2 SeitenAvi Kremer Case AnalysisSurya BakshiNoch keine Bewertungen
- Janie Jacobs Resume March 2019Dokument2 SeitenJanie Jacobs Resume March 2019api-404179099Noch keine Bewertungen
- Bumrungrad HospitalDokument3 SeitenBumrungrad HospitalAhmadnur kholilNoch keine Bewertungen
- JaundiceDokument53 SeitenJaundiceAbhishiktaAbhiNoch keine Bewertungen
- Ingle's EndodonticsDokument35 SeitenIngle's EndodonticsAndrei AntipinNoch keine Bewertungen
- Abnormal Behavior in Historical Context Prepared By: Miss Norzihan AyubDokument43 SeitenAbnormal Behavior in Historical Context Prepared By: Miss Norzihan AyubHanin Syahira HazahaNoch keine Bewertungen
- Health Care Industry Crystal Report ScenariosDokument2 SeitenHealth Care Industry Crystal Report ScenariosKishore KumarNoch keine Bewertungen
- Exodus SMLXL Rem KoolhaasDokument11 SeitenExodus SMLXL Rem Koolhaasjako60Noch keine Bewertungen
- ORTHOPAEDICS TRAUMADokument33 SeitenORTHOPAEDICS TRAUMARhomizal MazaliNoch keine Bewertungen
- Infectious Diseases Consultation ReportDokument5 SeitenInfectious Diseases Consultation ReportRohitKumar100% (1)
- IV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneDokument2 SeitenIV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneNdalilashiwa Penehafo Ndakondja-VictorNoch keine Bewertungen
- FINALS TheoreticalDokument6 SeitenFINALS TheoreticalCarol Neng Calupitan100% (1)
- Safe Blood UseDokument2 SeitenSafe Blood UseAnnette LowryNoch keine Bewertungen
- Freud Constructions in AnalysisDokument9 SeitenFreud Constructions in AnalysisyaelfridNoch keine Bewertungen
- Tumor ImmunologyDokument3 SeitenTumor ImmunologyStaz Reiya KiraNoch keine Bewertungen
- IMNCI Students Handbook PDFDokument93 SeitenIMNCI Students Handbook PDFAamira Qureshi100% (4)
- Selected Papers On Hysteria and Other PsychoneurosesDokument4 SeitenSelected Papers On Hysteria and Other PsychoneurosesAaron GroeblNoch keine Bewertungen
- ICNCDRS Blindness Registry FormDokument4 SeitenICNCDRS Blindness Registry FormAprilAngeliRobleNoch keine Bewertungen
- Dr. Steven Corwin LetterDokument2 SeitenDr. Steven Corwin LetterJonathan LaMantiaNoch keine Bewertungen
- Presented by - LALITA Sharma Msc. Nursing 1 YearDokument34 SeitenPresented by - LALITA Sharma Msc. Nursing 1 YearLalita SharmaNoch keine Bewertungen