Das könnte Ihnen auch gefallen
- Comprehensive Geriatric AssessmentDokument25 SeitenComprehensive Geriatric Assessmentsantosestrella100% (6)
- BSC PT - General Physiotherapy Assessent FormDokument2 SeitenBSC PT - General Physiotherapy Assessent Formrambabs3690% (1)
- BSC PT - Patient Assessment GuidelinesDokument13 SeitenBSC PT - Patient Assessment Guidelinesrambabs369Noch keine Bewertungen
- Check ListDokument1 SeiteCheck Listrambabs369Noch keine Bewertungen
- General Anatomy of The: Male Reproductive SystemDokument13 SeitenGeneral Anatomy of The: Male Reproductive Systemrambabs369100% (1)
- BSC PT - Patient Consent Form For ClinicDokument2 SeitenBSC PT - Patient Consent Form For Clinicrambabs369Noch keine Bewertungen
- European Core Standards of Physiotherapy PracticeDokument43 SeitenEuropean Core Standards of Physiotherapy Practicerambabs369Noch keine Bewertungen
- Credit Hour Calculation-MQA SAMPLEDokument38 SeitenCredit Hour Calculation-MQA SAMPLEYin Kit100% (1)
- BSC PT - Cultureal Competence in PT PracticeDokument25 SeitenBSC PT - Cultureal Competence in PT Practicerambabs369Noch keine Bewertungen
- BSC PT - Inpatient PT Evaluation FormDokument1 SeiteBSC PT - Inpatient PT Evaluation Formrambabs369100% (1)
- Resume From Ramesh Babu ManivannanDokument14 SeitenResume From Ramesh Babu Manivannanrambabs369Noch keine Bewertungen
- Clinic BannerDokument1 SeiteClinic Bannerrambabs369Noch keine Bewertungen
- Intramembranous Ossification: Process Diagrams Step-by-StepDokument5 SeitenIntramembranous Ossification: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Effects of Human Growth Hormone: Process Diagrams Step-by-StepDokument11 SeitenEffects of Human Growth Hormone: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- General Anatomy of The Immune SystemDokument29 SeitenGeneral Anatomy of The Immune Systemrambabs369100% (2)
- How An Enzyme Works: Process Diagrams Step-by-StepDokument4 SeitenHow An Enzyme Works: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Introductio To:: SplanchnologyDokument36 SeitenIntroductio To:: Splanchnologyrambabs369Noch keine Bewertungen
- The Contraction Cycle: Process Diagrams Step-by-StepDokument5 SeitenThe Contraction Cycle: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Facilitated Diffusion of Glucose: Process Diagrams Step-by-StepDokument4 SeitenFacilitated Diffusion of Glucose: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
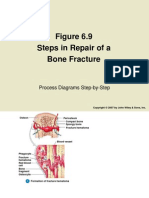
- Steps in Repair of A Bone Fracture: Process Diagrams Step-by-StepDokument5 SeitenSteps in Repair of A Bone Fracture: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Protein Elongation and Termination: Process Diagrams Step-by-StepDokument7 SeitenProtein Elongation and Termination: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Steps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-StepDokument9 SeitenSteps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Cell Division: Mitosis and Cytokinesis: Process Diagrams Step-by-StepDokument7 SeitenCell Division: Mitosis and Cytokinesis: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- ARTHOLOGYDokument38 SeitenARTHOLOGYrambabs369Noch keine Bewertungen
- Receptor-Mediated Endocytosis: Process Diagrams Step-by-StepDokument7 SeitenReceptor-Mediated Endocytosis: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Skeletal and muscular system overviewDokument86 SeitenSkeletal and muscular system overviewrambabs369Noch keine Bewertungen
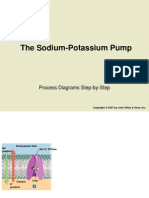
- The Sodium-Potassium Pump: Process Diagrams Step-by-StepDokument5 SeitenThe Sodium-Potassium Pump: Process Diagrams Step-by-Steprambabs369Noch keine Bewertungen
- Chapter One Introduction To PathologyDokument26 SeitenChapter One Introduction To Pathologyrambabs369Noch keine Bewertungen
- Time Off SlipDokument1 SeiteTime Off Sliprambabs369Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Being Afraid: Everyday WorriesDokument10 SeitenBeing Afraid: Everyday Worriesdina171279Noch keine Bewertungen
- HmisDokument14 SeitenHmis166873100% (1)
- B.+BraunSpace 6064516 Pocket Guide PDFDokument8 SeitenB.+BraunSpace 6064516 Pocket Guide PDFsusiloNoch keine Bewertungen
- Related Coverage: Stigma Experienced by Children and Adolescents With Obesity Use Neutral WordsDokument5 SeitenRelated Coverage: Stigma Experienced by Children and Adolescents With Obesity Use Neutral WordsSlaghard AnerajNoch keine Bewertungen
- CYTOCHROME P450 DRUG INTERACTION TABLE - Drug InteractionsDokument19 SeitenCYTOCHROME P450 DRUG INTERACTION TABLE - Drug InteractionsAna MurielNoch keine Bewertungen
- 10 1 1 947 3241Dokument8 Seiten10 1 1 947 3241Mayur MulyeNoch keine Bewertungen
- Carob (Ceratonia siliqua): Mechanism of Action and PharmacologyDokument7 SeitenCarob (Ceratonia siliqua): Mechanism of Action and PharmacologyMonica BotaNoch keine Bewertungen
- CrohnsDokument19 SeitenCrohnsLauren LevyNoch keine Bewertungen
- Additive Substances in Doping: State University of JakartaDokument11 SeitenAdditive Substances in Doping: State University of Jakartatiaranbl2023Noch keine Bewertungen
- Health Promotion Methods and ApproachesDokument18 SeitenHealth Promotion Methods and ApproachesDrGagandeep Singh100% (1)
- Drug StudyDokument5 SeitenDrug StudyRai D. MacapantonNoch keine Bewertungen
- PUBOurWaterOurFuture PDFDokument52 SeitenPUBOurWaterOurFuture PDFjossNoch keine Bewertungen
- Complete Urinalysis: A. Physical Characteristics of UrineDokument8 SeitenComplete Urinalysis: A. Physical Characteristics of UrineKryza Dale Bunado BaticanNoch keine Bewertungen
- EFN - PPTX 3Dokument9 SeitenEFN - PPTX 3Suheni Khotimah IndrianiNoch keine Bewertungen
- BDD Module 2 - Maintenance2 PDFDokument14 SeitenBDD Module 2 - Maintenance2 PDFHemant KumarNoch keine Bewertungen
- Colonic InertiaDokument20 SeitenColonic InertiaAndina Destiyani PutriNoch keine Bewertungen
- KNH 413 Case Study 4Dokument12 SeitenKNH 413 Case Study 4api-272540385100% (1)
- Families of Children With Special Needs 0909Dokument8 SeitenFamilies of Children With Special Needs 0909Mary Florilyn ReclaNoch keine Bewertungen
- Temporomandibular Joint DisorderDokument9 SeitenTemporomandibular Joint DisorderTannels100% (1)
- The EyeDokument8 SeitenThe Eyezyrine jhen100% (1)
- Surgical Staplers: Circular / Linear / PPH / Linear CutterDokument24 SeitenSurgical Staplers: Circular / Linear / PPH / Linear CutterRino KefasNoch keine Bewertungen
- Soap Note Template 33Dokument3 SeitenSoap Note Template 33Rafael G. Garcia SanchezNoch keine Bewertungen
- Category-Wise Opening & Closing Rank-Ayur - BHU Int.Dokument5 SeitenCategory-Wise Opening & Closing Rank-Ayur - BHU Int.srikanth PosaNoch keine Bewertungen
- Enviro-Flo, Inc. Enviro-Chlor Tablet Chlorinator: Installation & Owner'S ManualDokument7 SeitenEnviro-Flo, Inc. Enviro-Chlor Tablet Chlorinator: Installation & Owner'S ManualSteve DennisNoch keine Bewertungen
- An Update On The Management of Endometrial HyperplasiaDokument5 SeitenAn Update On The Management of Endometrial Hyperplasiafitrah fajrianiNoch keine Bewertungen
- Case #2: Group CDokument27 SeitenCase #2: Group CKartik SharmaNoch keine Bewertungen
- Feeding larvae to predatory bug nymphsDokument4 SeitenFeeding larvae to predatory bug nymphsEvawaty Sri UlinaNoch keine Bewertungen
- Case Group 1Dokument10 SeitenCase Group 1JASMEEN RAVALNoch keine Bewertungen
- Yakima Co (WA) Protocols 2010Dokument117 SeitenYakima Co (WA) Protocols 2010Anthony James-Hartwell100% (1)
- HYper and Hypo TGDokument43 SeitenHYper and Hypo TGRiajoy AsisNoch keine Bewertungen