Das könnte Ihnen auch gefallen
- 10 - "Crown-then-Graft" - A Novel Approach To OptimizeDokument14 Seiten10 - "Crown-then-Graft" - A Novel Approach To OptimizePablo BenitezNoch keine Bewertungen
- 2006 Use of Additive PDFDokument10 Seiten2006 Use of Additive PDFVipul SrivastavaNoch keine Bewertungen
- Clinical Aid OyDokument7 SeitenClinical Aid OyFriadi NataNoch keine Bewertungen
- 11 Cavity PreparationsDokument13 Seiten11 Cavity PreparationsMarco Miranda RodríguezNoch keine Bewertungen
- A New Concept in Maintaining The Emergence ProfileDokument8 SeitenA New Concept in Maintaining The Emergence ProfileankitaNoch keine Bewertungen
- Bringing Composite To An Art Form in The Anterior SegmentDokument4 SeitenBringing Composite To An Art Form in The Anterior SegmentMohamed Ibrahem MohamedNoch keine Bewertungen
- Simon Magne Mockup 2008Dokument8 SeitenSimon Magne Mockup 2008George PapaemmanouilNoch keine Bewertungen
- A Direct Composite Resin Stratification Technique For Restoration PDFDokument8 SeitenA Direct Composite Resin Stratification Technique For Restoration PDFjuanNoch keine Bewertungen
- Fernandesdacunha 2017Dokument7 SeitenFernandesdacunha 2017Mauricio Hernández ValdezNoch keine Bewertungen
- Starb Urst BevelDokument4 SeitenStarb Urst BevelventynataliaNoch keine Bewertungen
- Planeamiento DiagnosticoDokument15 SeitenPlaneamiento DiagnosticoJuan Andres EspinozaNoch keine Bewertungen
- 1-s2.0-S027823911630502X-main 2Dokument8 Seiten1-s2.0-S027823911630502X-main 2beautopia reviewsNoch keine Bewertungen
- Preplanned Surgical Obturator Prosthesis - A Boon For RehabilitationDokument6 SeitenPreplanned Surgical Obturator Prosthesis - A Boon For RehabilitationVero AngelNoch keine Bewertungen
- RSGDokument5 SeitenRSGHugoMoralesTecnicoDentalNoch keine Bewertungen
- Ijss Feb Ra01Dokument5 SeitenIjss Feb Ra01Ruxandra FitaNoch keine Bewertungen
- Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewDokument9 SeitenAdhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewAbdelrahman GalalNoch keine Bewertungen
- 2011 EJED DitramaxDokument10 Seiten2011 EJED DitramaxPabloSevillaHernandezNoch keine Bewertungen
- BoptloiDokument14 SeitenBoptloiSonea M100% (1)
- Esthetic Rehabilitation of A Severely Worn Dentition With MIPPDokument22 SeitenEsthetic Rehabilitation of A Severely Worn Dentition With MIPPKarla Margine PérezNoch keine Bewertungen
- ROA Scopin 2014 4Dokument24 SeitenROA Scopin 2014 4Patrick Castillo SalazarNoch keine Bewertungen
- 3D - Printed Crowns - Cost EffectiveDokument4 Seiten3D - Printed Crowns - Cost EffectiveLuis Felipe SchneiderNoch keine Bewertungen
- The Stamp Technique For Direct Composite RestorationsDokument4 SeitenThe Stamp Technique For Direct Composite RestorationsIJAR JOURNALNoch keine Bewertungen
- Cosmetic Dentistry CSD 2013Dokument3 SeitenCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNoch keine Bewertungen
- Protocolo Rehabilitacion OralDokument25 SeitenProtocolo Rehabilitacion Oraljotapintor100% (8)
- Composite Resin Layering and Placement TechniquesDokument7 SeitenComposite Resin Layering and Placement TechniquesenimaNoch keine Bewertungen
- The Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethDokument18 SeitenThe Scalpel Finishing Technique: A Tooth-Friendly Way To Finish Dental Composites in Anterior TeethSoraya BouchammaNoch keine Bewertungen
- Ijomi 15 272Dokument6 SeitenIjomi 15 272Bagis Emre GulNoch keine Bewertungen
- Surgical Orthodontic Cephalometric Prediction TracingDokument8 SeitenSurgical Orthodontic Cephalometric Prediction TracingMariyamNoch keine Bewertungen
- Teeth in A Day Nys deDokument4 SeitenTeeth in A Day Nys deSatyendra KumarNoch keine Bewertungen
- Repairing Worn Dentition: MasterclassDokument5 SeitenRepairing Worn Dentition: MasterclassAlfredo RamzNoch keine Bewertungen
- Teflon Tape TechniqueDokument6 SeitenTeflon Tape TechniqueJuan K. J. Shin100% (1)
- Technical Aspects of Complete Denture Construction: ProstheticsDokument4 SeitenTechnical Aspects of Complete Denture Construction: ProstheticsNaveen S YadavNoch keine Bewertungen
- Minimall Tooth Preparation Garil GurelDokument13 SeitenMinimall Tooth Preparation Garil GurelMónica BecerraNoch keine Bewertungen
- Direct Post Composite09Dokument16 SeitenDirect Post Composite09hmsatNoch keine Bewertungen
- Rde 39 24Dokument8 SeitenRde 39 24pyrockerNoch keine Bewertungen
- The Hybrid Denture1Dokument9 SeitenThe Hybrid Denture1SitiKhadijah100% (1)
- Direct Restoration of Anterior TeethDokument9 SeitenDirect Restoration of Anterior TeethbubbiexoNoch keine Bewertungen
- Implant DentistryDokument196 SeitenImplant DentistryAkanksha MahajanNoch keine Bewertungen
- 11 - Soft Tissue Waxup and Mock-Up and Key Factors inDokument15 Seiten11 - Soft Tissue Waxup and Mock-Up and Key Factors inPablo BenitezNoch keine Bewertungen
- Closing Open Contacts Adjacent To An Implant-SuppoDokument3 SeitenClosing Open Contacts Adjacent To An Implant-SuppoSeptimiu TiplicaNoch keine Bewertungen
- ADokument8 SeitenARaghava DasariNoch keine Bewertungen
- Posterior CompositeDokument21 SeitenPosterior CompositeNaji Z. ArandiNoch keine Bewertungen
- Amalgam Carving TechniqueDokument5 SeitenAmalgam Carving Techniquearun3883Noch keine Bewertungen
- Preprosthetic Surgery in The ElderlyDokument8 SeitenPreprosthetic Surgery in The ElderlybkprosthoNoch keine Bewertungen
- Preoperative View of A DiastemaDokument6 SeitenPreoperative View of A Diastemaulfa rizalniNoch keine Bewertungen
- 10 1016@j Cden 2007 03 007 PDFDokument13 Seiten10 1016@j Cden 2007 03 007 PDFsnehal jaiswalNoch keine Bewertungen
- CADCAM Splints For The Functional and Esthetic, DANIEL EDELHOFFDokument12 SeitenCADCAM Splints For The Functional and Esthetic, DANIEL EDELHOFFFreddy BenalcázarNoch keine Bewertungen
- Aesthetic Layering TechniqueDokument0 SeitenAesthetic Layering Techniqueatul_singh2001Noch keine Bewertungen
- Intra Oral A Cry y Lic SplintsDokument17 SeitenIntra Oral A Cry y Lic SplintsGreat PotatosNoch keine Bewertungen
- CLP Surgical GuideDokument3 SeitenCLP Surgical GuideAmit SadhwaniNoch keine Bewertungen
- Facial Analysis. A Chomprensyve Approach To Treatment Planning in Ahesthetic DentistryDokument8 SeitenFacial Analysis. A Chomprensyve Approach To Treatment Planning in Ahesthetic DentistryOmanakuttan KrNoch keine Bewertungen
- Initial Prosthetic TreatmentDokument10 SeitenInitial Prosthetic TreatmentMohsin HabibNoch keine Bewertungen
- CAD CAM Splints For The Functional and Esthetic Evaluation of Newly Defined Occlusal Dimensions PDFDokument12 SeitenCAD CAM Splints For The Functional and Esthetic Evaluation of Newly Defined Occlusal Dimensions PDFEsme ValenciaNoch keine Bewertungen
- IJEDe 18 04 Fabbri 1261 4Dokument15 SeitenIJEDe 18 04 Fabbri 1261 4Eduardo CepedaNoch keine Bewertungen
- Establishing The Posterior Palatal Seal During The Final Impression StageDokument3 SeitenEstablishing The Posterior Palatal Seal During The Final Impression Stageرلا رةنNoch keine Bewertungen
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsVon EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNoch keine Bewertungen
- Treatment Planning Single Maxillary Anterior Implants for DentistsVon EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNoch keine Bewertungen
- Stress, Allostatic Load, and Periodontal DiseasesDokument8 SeitenStress, Allostatic Load, and Periodontal DiseasesRuxandra MurariuNoch keine Bewertungen
- Periodontal Complications of Prescription and Recreational DDokument12 SeitenPeriodontal Complications of Prescription and Recreational DRuxandra MurariuNoch keine Bewertungen
- Curs Inhalo 3Dokument39 SeitenCurs Inhalo 3Ruxandra MurariuNoch keine Bewertungen
- 21 Principles Smile Design Lee OstlerDokument43 Seiten21 Principles Smile Design Lee OstlerRuxandra Murariu100% (7)
- AMC Mining Brochure (A4 LR)Dokument2 SeitenAMC Mining Brochure (A4 LR)Bandung WestNoch keine Bewertungen
- Trigger: Business Process Procedure OverviewDokument11 SeitenTrigger: Business Process Procedure Overviewcalalitbajaj100% (1)
- Id or Class Are SimplyDokument5 SeitenId or Class Are SimplyK CorNoch keine Bewertungen
- Packing Shipping InstructionsDokument2 SeitenPacking Shipping InstructionsJ.V. Siritt ChangNoch keine Bewertungen
- Caso 1 - Tunel Sismico BoluDokument4 SeitenCaso 1 - Tunel Sismico BoluCarlos Catalán CórdovaNoch keine Bewertungen
- 20779A ENU CompanionDokument86 Seiten20779A ENU Companionmiamikk204Noch keine Bewertungen
- Method Statement: Vetotop XT539Dokument4 SeitenMethod Statement: Vetotop XT539محمد عزتNoch keine Bewertungen
- Electric Baseboard StelproDokument4 SeitenElectric Baseboard StelprojrodNoch keine Bewertungen
- Method Statement Footing - PDF - Concrete - Deep FoundationDokument12 SeitenMethod Statement Footing - PDF - Concrete - Deep FoundationJYDP RNoch keine Bewertungen
- MCA Proposal For OutsourcingDokument2 SeitenMCA Proposal For OutsourcingLazaros KarapouNoch keine Bewertungen
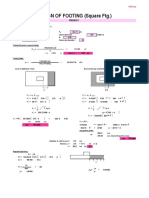
- Design of Footing (Square FTG.) : M Say, L 3.75Dokument2 SeitenDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNoch keine Bewertungen
- A Survey Report On The Preferred RestaurDokument22 SeitenA Survey Report On The Preferred RestaurEIGHA & ASHLEIGH EnriquezNoch keine Bewertungen
- DS TEGO Polish Additiv WE 50 e 1112Dokument3 SeitenDS TEGO Polish Additiv WE 50 e 1112Noelia Gutiérrez CastroNoch keine Bewertungen
- Application For Leave - EODokument1 SeiteApplication For Leave - EOcomelec carmenNoch keine Bewertungen
- Technical BidDokument64 SeitenTechnical Bidjhon smithNoch keine Bewertungen
- Cooling Gas Compressor: Cable ListDokument4 SeitenCooling Gas Compressor: Cable ListHaitham YoussefNoch keine Bewertungen
- Enhancing LAN Using CryptographyDokument2 SeitenEnhancing LAN Using CryptographyMonim Moni100% (1)
- APCJ Directory 2019Dokument34 SeitenAPCJ Directory 2019Anonymous Pu3OF7100% (3)
- Thematic CodingDokument31 SeitenThematic CodingLance Jazekmiel DOMINGONoch keine Bewertungen
- Link Belt Rec Parts LastDokument15 SeitenLink Belt Rec Parts LastBishoo ShenoudaNoch keine Bewertungen
- Muster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINDokument9 SeitenMuster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINwwaallNoch keine Bewertungen
- Microstrip Antennas: How Do They Work?Dokument2 SeitenMicrostrip Antennas: How Do They Work?Tebogo SekgwamaNoch keine Bewertungen
- Gabuyer Oct13Dokument72 SeitenGabuyer Oct13William Rios0% (1)
- Consumer Behaviour Models in Hospitality and TourismDokument16 SeitenConsumer Behaviour Models in Hospitality and Tourismfelize padllaNoch keine Bewertungen
- Employee Involvement TQMDokument33 SeitenEmployee Involvement TQMAli RazaNoch keine Bewertungen
- SC Circular Re BP 22 Docket FeeDokument2 SeitenSC Circular Re BP 22 Docket FeeBenjamin HaysNoch keine Bewertungen
- Move It 3. Test U3Dokument2 SeitenMove It 3. Test U3Fabian AmayaNoch keine Bewertungen
- Raport de Incercare TL 82 Engleza 2015 MasticDokument3 SeitenRaport de Incercare TL 82 Engleza 2015 MasticRoxana IoanaNoch keine Bewertungen
- MBA-CM - ME - Lecture 16 Market Structure AnalysisDokument11 SeitenMBA-CM - ME - Lecture 16 Market Structure Analysisrohan_solomonNoch keine Bewertungen
- Tutorial 1 Process Heat TransferDokument4 SeitenTutorial 1 Process Heat TransferSuraya JohariNoch keine Bewertungen