Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- BS en 50216-6 2002Dokument18 SeitenBS en 50216-6 2002Jeff Anderson Collins100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Sunrise - 12 AB-unlockedDokument81 SeitenSunrise - 12 AB-unlockedMohamed Thanoon50% (2)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- RMC No. 122 2022 9.6.2022Dokument6 SeitenRMC No. 122 2022 9.6.2022RUFO BULILANNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- NST 029Dokument123 SeitenNST 029Riaz Ahmad BhattiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Reclaimer PDFDokument8 SeitenReclaimer PDFSiti NurhidayatiNoch keine Bewertungen
- Neural Computing and ApplicationsDokument49 SeitenNeural Computing and ApplicationsLine PhamNoch keine Bewertungen
- Jack Arch RetrofitDokument13 SeitenJack Arch RetrofitDebendra Dev KhanalNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Ccie R&s Expanded-BlueprintDokument12 SeitenCcie R&s Expanded-BlueprintAftab AlamNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Blackstone The Dash Model #1610 Owner's ManualDokument53 SeitenBlackstone The Dash Model #1610 Owner's ManualSydney Adam SteeleNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Lecture Notes - Introduction To Big DataDokument8 SeitenLecture Notes - Introduction To Big Datasakshi kureley0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Nielsen Report - The New Trend Among Indonesia's NetizensDokument20 SeitenNielsen Report - The New Trend Among Indonesia's NetizensMarsha ImaniaraNoch keine Bewertungen
- CSCI 123 - Final ExamDokument15 SeitenCSCI 123 - Final ExamBrianYoungNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- FDP VLSI Design at Deep Submicron Node PDFDokument2 SeitenFDP VLSI Design at Deep Submicron Node PDFpraneethshubNoch keine Bewertungen
- American J of Comm Psychol - 2023 - Palmer - Looted Artifacts and Museums Perpetuation of Imperialism and RacismDokument9 SeitenAmerican J of Comm Psychol - 2023 - Palmer - Looted Artifacts and Museums Perpetuation of Imperialism and RacismeyeohneeduhNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- SPWM Vs SVMDokument11 SeitenSPWM Vs SVMpmbalajibtechNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Making of A Scientist Class 10Dokument2 SeitenThe Making of A Scientist Class 10abhigna.ravikumarNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- L Rexx PDFDokument9 SeitenL Rexx PDFborisg3Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Model Personal StatementDokument2 SeitenModel Personal StatementSwayam Tripathy100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Python Cheat Sheet-1Dokument8 SeitenPython Cheat Sheet-1RevathyNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Contract 1 ProjectDokument21 SeitenContract 1 ProjectAditi BanerjeeNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Tournament Rules and MechanicsDokument2 SeitenTournament Rules and MechanicsMarkAllenPascualNoch keine Bewertungen
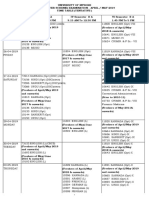
- Ugtt April May 2019 NewDokument48 SeitenUgtt April May 2019 NewSuhas SNoch keine Bewertungen
- Introduction To Templates in C++Dokument16 SeitenIntroduction To Templates in C++hammarbytpNoch keine Bewertungen
- Assembly and RiggingDokument52 SeitenAssembly and RiggingPokemon Go0% (1)
- Portland Cement: Standard Specification ForDokument9 SeitenPortland Cement: Standard Specification ForHishmat Ezz AlarabNoch keine Bewertungen
- Project ProposalDokument2 SeitenProject Proposalqueen malik80% (5)
- 3Dokument76 Seiten3Uday ShankarNoch keine Bewertungen
- Organic Logo-Faq enDokument6 SeitenOrganic Logo-Faq enjcnavarro_Noch keine Bewertungen
- 96 Dec2018 NZGeoNews PDFDokument139 Seiten96 Dec2018 NZGeoNews PDFAditya PrasadNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- BIO122 - CHAPTER 7 Part 1Dokument53 SeitenBIO122 - CHAPTER 7 Part 1lili100% (1)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)