Das könnte Ihnen auch gefallen
- Illustrations Of Special Effective Acupoints for common DiseasesVon EverandIllustrations Of Special Effective Acupoints for common DiseasesNoch keine Bewertungen
- Basic Characteristics of TCMDokument47 SeitenBasic Characteristics of TCMEINSTEIN2DNoch keine Bewertungen
- New Approach to Treating Female Infertility Integrates Chinese and Western MedicineDokument23 SeitenNew Approach to Treating Female Infertility Integrates Chinese and Western Medicinean ssiNoch keine Bewertungen
- Fertility Acupuncture NJDokument1 SeiteFertility Acupuncture NJJaceyNoch keine Bewertungen
- The Acupuncture Prescription:: A Holistic Approach to HealthVon EverandThe Acupuncture Prescription:: A Holistic Approach to HealthNoch keine Bewertungen
- Cham Cuu Dong Thi Dieu Tri CA Benh KhoDokument111 SeitenCham Cuu Dong Thi Dieu Tri CA Benh KhoTrieu VuongNoch keine Bewertungen
- Compilation Conditions + FormulasDokument2 SeitenCompilation Conditions + Formulaspeter911x0% (1)
- Traditional Chinese Medicine Initial Consultation FormDokument5 SeitenTraditional Chinese Medicine Initial Consultation Formbob100% (1)
- 6 Acupuncture and GynecologyDokument98 Seiten6 Acupuncture and GynecologyKiran PhalkeNoch keine Bewertungen
- 2017 Acupuncture For Chronic PainDokument49 Seiten2017 Acupuncture For Chronic Painvera100% (1)
- Diabetes MellitusDokument8 SeitenDiabetes Mellitusab21423Noch keine Bewertungen
- GlaucomaDokument6 SeitenGlaucomaratamanoNoch keine Bewertungen
- Aasp Section 3 ShowDokument105 SeitenAasp Section 3 ShowLakshmigiNoch keine Bewertungen
- Tran MentalactivityDokument33 SeitenTran MentalactivityKiran JoshiNoch keine Bewertungen
- TCM Acupuncture Theory - ... Points - Yin Yang HouseDokument2 SeitenTCM Acupuncture Theory - ... Points - Yin Yang Houseabx5002Noch keine Bewertungen
- Li Shizhen and The Grand Compendium of Materia MedDokument2 SeitenLi Shizhen and The Grand Compendium of Materia MedLương Ngọc TúNoch keine Bewertungen
- A Clinician's Guide To Using Granule ExtractsDokument252 SeitenA Clinician's Guide To Using Granule ExtractsSalsa Nabila AwliaNoch keine Bewertungen
- Acupuncture For Treatment of Irritable Bowel SyndromeDokument40 SeitenAcupuncture For Treatment of Irritable Bowel SyndromeTomas MascaroNoch keine Bewertungen
- Alchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMDokument3 SeitenAlchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMHaryono zhuNoch keine Bewertungen
- TCM Diabetes Seminar NotesDokument30 SeitenTCM Diabetes Seminar Notespranaji100% (1)
- Diabetes Perspectives and TreatmentsDokument32 SeitenDiabetes Perspectives and TreatmentsyellahfellahNoch keine Bewertungen
- DR Men's Chinese Sublingual Dia - Beijing MenDokument52 SeitenDR Men's Chinese Sublingual Dia - Beijing Menalejandromlopez100% (1)
- Guidelines For Formulating A TCM DiagnosisDokument8 SeitenGuidelines For Formulating A TCM DiagnosisNiltonNoch keine Bewertungen
- Acupuncture For ObesityDokument2 SeitenAcupuncture For ObesityGermán Mariano Torrez G100% (1)
- Disorders of BloodDokument9 SeitenDisorders of BloodRoberto BigliaNoch keine Bewertungen
- Treatment of Benign Prostatic Hyperplasia and Erectile Dysfunction PDFDokument191 SeitenTreatment of Benign Prostatic Hyperplasia and Erectile Dysfunction PDFMontserratNoch keine Bewertungen
- Training Course Mumbai June 2013 & Correspondence CoursesDokument9 SeitenTraining Course Mumbai June 2013 & Correspondence CoursesJenneey D RajaniNoch keine Bewertungen
- Acupuncture Accordind Traditional PHDDokument13 SeitenAcupuncture Accordind Traditional PHDcugarNoch keine Bewertungen
- Skin Diseases 1. Urticaria: I. Standard TreatmentDokument23 SeitenSkin Diseases 1. Urticaria: I. Standard TreatmentMonsecita EsnowNoch keine Bewertungen
- Qi, Blood, and Body FluidsDokument81 SeitenQi, Blood, and Body FluidsFatimah OthmanNoch keine Bewertungen
- The Use of Acupuncture and Modern Techniques in The Treatment of CancerDokument29 SeitenThe Use of Acupuncture and Modern Techniques in The Treatment of CancerRoni SapirNoch keine Bewertungen
- Impotence Chart FinalDokument2 SeitenImpotence Chart FinalKaty Firisin100% (1)
- Intro To Scalp Acupuncture - 25 Pages PDFDokument25 SeitenIntro To Scalp Acupuncture - 25 Pages PDFafisioterapia100% (5)
- 2008 Acupuncture Core Therapy - ToCDokument15 Seiten2008 Acupuncture Core Therapy - ToCdoktormin106100% (1)
- Miyawaki Yuki Kuwahara Koei Hari Handbook of Traditional JapDokument23 SeitenMiyawaki Yuki Kuwahara Koei Hari Handbook of Traditional Japкостя100% (1)
- MK Sastry .Fundamentals of TCM DiagnosticsDokument148 SeitenMK Sastry .Fundamentals of TCM DiagnosticsEdison halim100% (1)
- Obesity - Causes and Treatment OptionsDokument3 SeitenObesity - Causes and Treatment OptionsPirasan Traditional Medicine CenterNoch keine Bewertungen
- Acupuncture Theory - OdtDokument2 SeitenAcupuncture Theory - OdtAyyush RajalingaNoch keine Bewertungen
- Raphael Rettner - 5 Ways To Lose 10 Lbs. in 30 DaysDokument29 SeitenRaphael Rettner - 5 Ways To Lose 10 Lbs. in 30 DaysYuldash100% (1)
- Auricular Seed Therapy To Improve SleepDokument2 SeitenAuricular Seed Therapy To Improve SleepBenito Camelas LopezNoch keine Bewertungen
- How Chinese Medicine Views the Relationship Between Emotions, Physiology and the Minister FireDokument7 SeitenHow Chinese Medicine Views the Relationship Between Emotions, Physiology and the Minister FireRicardo TeixeiraNoch keine Bewertungen
- Acupuncture For SchizophreniaDokument28 SeitenAcupuncture For SchizophreniaTomas MascaroNoch keine Bewertungen
- Cheng AcupunctureforWomenwithObesity PDFDokument13 SeitenCheng AcupunctureforWomenwithObesity PDFAshari Fisio180% (1)
- DR Tans Balance Method PDFDokument18 SeitenDR Tans Balance Method PDFJoy Arguelles GoolNoch keine Bewertungen
- Acupuncture Treatment of AsthmaDokument20 SeitenAcupuncture Treatment of AsthmafrankgzlNoch keine Bewertungen
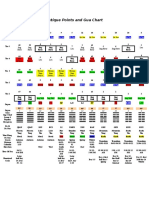
- Ancient Chinese Gua Chart and Organ PointsDokument1 SeiteAncient Chinese Gua Chart and Organ PointsPedro MaiaNoch keine Bewertungen
- CALE Formulas 83 BestDokument119 SeitenCALE Formulas 83 BestAyanna CobbNoch keine Bewertungen
- CMAC121 Point Location: Session 2 Hand Tai Yin (Lung) ChannelDokument24 SeitenCMAC121 Point Location: Session 2 Hand Tai Yin (Lung) ChannelvinayNoch keine Bewertungen
- Daoyin 12 Methods - 19th June Pukekohe PDFDokument1 SeiteDaoyin 12 Methods - 19th June Pukekohe PDFwushu_worksNoch keine Bewertungen
- Wrist and Ankle Acupuncture Book, by Josep CarrionDokument199 SeitenWrist and Ankle Acupuncture Book, by Josep Carrionjosep100% (1)
- Traditional Chinese Medicine Resource Guide: Key Herbs, Formulas & HistoryDokument103 SeitenTraditional Chinese Medicine Resource Guide: Key Herbs, Formulas & HistoryBrian LiNoch keine Bewertungen
- Modern and Traditional Chinese Approaches to DiabetesDokument10 SeitenModern and Traditional Chinese Approaches to DiabetesGabriel Navarro100% (1)
- Neoclassical Acupuncture and a Childhood CallingDokument13 SeitenNeoclassical Acupuncture and a Childhood CallingzhikNoch keine Bewertungen
- Dkendall Mechanismsofacup LNDokument70 SeitenDkendall Mechanismsofacup LNJohnNoch keine Bewertungen
- Evidence Summary - Pediatric AcupunctureDokument14 SeitenEvidence Summary - Pediatric AcupunctureyayanicaNoch keine Bewertungen
- Cwang Tungfemale LN TCMWTDokument14 SeitenCwang Tungfemale LN TCMWTdrprasant50% (2)
- Evidence Based AcupunctureDokument6 SeitenEvidence Based Acupuncturerajveej99Noch keine Bewertungen
- Managing Pain: And Other Medically Proven Uses of AcupunctureVon EverandManaging Pain: And Other Medically Proven Uses of AcupunctureNoch keine Bewertungen
- Brainmap ChanDokument29 SeitenBrainmap ChanChandra MosesNoch keine Bewertungen
- Playstation-3-Cechl04 Service ManualDokument0 SeitenPlaystation-3-Cechl04 Service Manualpandorabox20120% (1)
- AcudDokument7 SeitenAcudDaniel Ramos GomezNoch keine Bewertungen
- Acupuncture Treatment TemporomandibularDokument21 SeitenAcupuncture Treatment Temporomandibularkazzascribd100% (2)
- EBM Journal Club Dysmenorrhea and AcupunctureDokument62 SeitenEBM Journal Club Dysmenorrhea and AcupunctureChandra MosesNoch keine Bewertungen
- The Safe Use of Difficult and Dangerous Acupuncture PointsDokument5 SeitenThe Safe Use of Difficult and Dangerous Acupuncture PointsChandra MosesNoch keine Bewertungen
- The Effect of Traditional Chinese Medical Acupuncture (TCM) On Test Anxiety (A Pilot Study)Dokument8 SeitenThe Effect of Traditional Chinese Medical Acupuncture (TCM) On Test Anxiety (A Pilot Study)Chandra MosesNoch keine Bewertungen
- Implementation and Organization of A Perioperative Lactation Program: A Descriptive StudyDokument9 SeitenImplementation and Organization of A Perioperative Lactation Program: A Descriptive StudypkmpsNoch keine Bewertungen
- F60 Turbine Operator Manual PDFDokument130 SeitenF60 Turbine Operator Manual PDFNoel SamNoch keine Bewertungen
- Carriere® SLX Patient EducationDokument2 SeitenCarriere® SLX Patient EducationOrtho OrganizersNoch keine Bewertungen
- CH 23 Respiration F 2017 SRMDokument153 SeitenCH 23 Respiration F 2017 SRMJuliaNoch keine Bewertungen
- pGALS - Paediatric Gait Arms Legs and Spine A PDFDokument7 SeitenpGALS - Paediatric Gait Arms Legs and Spine A PDFTeodor ŞişianuNoch keine Bewertungen
- 625-Naskah Artikel-1439-1-10-20190107Dokument11 Seiten625-Naskah Artikel-1439-1-10-20190107Dhany Nufikha LanasariNoch keine Bewertungen
- Trauma WajahDokument37 SeitenTrauma WajahdianNoch keine Bewertungen
- Guru Nanak Mission HospitalDokument16 SeitenGuru Nanak Mission HospitalAbhishek Singh Raghuvanshi100% (1)
- Doctors List for Sponsored PatientsDokument27 SeitenDoctors List for Sponsored PatientsAashwin PoovankunnilNoch keine Bewertungen
- ADV 11-12-15.9-FinalDokument1 SeiteADV 11-12-15.9-FinalWilliam Floyd School DistrictNoch keine Bewertungen
- 56 FullDokument63 Seiten56 FullLuca Selva CampobassoNoch keine Bewertungen
- CV NyeriDokument1 SeiteCV NyeriMuhammad YunusNoch keine Bewertungen
- Brosur EnglishDokument2 SeitenBrosur EnglishSumiari LuhNoch keine Bewertungen
- UntitledDokument7 SeitenUntitledapi-247066569Noch keine Bewertungen
- Access Cavity Preparation PDFDokument94 SeitenAccess Cavity Preparation PDFtomdienya100% (2)
- Ringerfundin e 03 07Dokument14 SeitenRingerfundin e 03 07Annisa KhairunnisaNoch keine Bewertungen
- DAFO 4 SoftyDokument1 SeiteDAFO 4 SoftyaliaskarNoch keine Bewertungen
- Cardiac Imaging Sept 2016tDokument254 SeitenCardiac Imaging Sept 2016tColeen Joyce NeyraNoch keine Bewertungen
- Gastric Carcinoid After Long-Term Use of A Proton Pump InhibitorDokument6 SeitenGastric Carcinoid After Long-Term Use of A Proton Pump InhibitorBpmStfbNoch keine Bewertungen
- Kista OvariumDokument4 SeitenKista OvariumAde Gustina SiahaanNoch keine Bewertungen
- Orthodontics PDFDokument6 SeitenOrthodontics PDFSusanth AlapatiNoch keine Bewertungen
- IHFG Part B Rehabilitation Allied HealthDokument19 SeitenIHFG Part B Rehabilitation Allied Healthamir alamNoch keine Bewertungen
- Effect of Lead Acetate On Spleen and Blood Parameters in Albino RatsDokument7 SeitenEffect of Lead Acetate On Spleen and Blood Parameters in Albino RatsInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Wrong Site, Wrong Side and Wrong Patient ProceduresDokument5 SeitenWrong Site, Wrong Side and Wrong Patient ProceduresDr Rajesh KalraNoch keine Bewertungen
- Olfactory MarketingDokument10 SeitenOlfactory MarketingjanpoolesgayNoch keine Bewertungen
- Parent Directed FeedingDokument3 SeitenParent Directed Feedingmichellis28Noch keine Bewertungen
- Al Lib 24.2012725923351516 PDFDokument2 SeitenAl Lib 24.2012725923351516 PDFFerdina NidyasariNoch keine Bewertungen
- Pediatric Assessment Physical ExamDokument9 SeitenPediatric Assessment Physical ExamBea SamonteNoch keine Bewertungen
- OCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004BradfordDokument244 SeitenOCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004Bradfordハルァン ファ烏山Noch keine Bewertungen
- Adult Echocardiography Protocol 14 2Dokument10 SeitenAdult Echocardiography Protocol 14 2api-349402240Noch keine Bewertungen