Das könnte Ihnen auch gefallen
- Sewing Machine Instruction ManualDokument30 SeitenSewing Machine Instruction ManualEric HubbardNoch keine Bewertungen
- Surface Contamination: Proceedings of a Symposium Held at Gatlinburg, Tennessee, June 1964Von EverandSurface Contamination: Proceedings of a Symposium Held at Gatlinburg, Tennessee, June 1964B. R. FishNoch keine Bewertungen
- Dental Implant CoatingDokument4 SeitenDental Implant Coatingkeyur_dholNoch keine Bewertungen
- Guidance For Industry and FDA Staff Class II Special Controls Guidance Document: Root Form Endosseous Dental Implants and Endosseous Dental AbutmentsDokument38 SeitenGuidance For Industry and FDA Staff Class II Special Controls Guidance Document: Root Form Endosseous Dental Implants and Endosseous Dental AbutmentsTomas Bras HarriottNoch keine Bewertungen
- Titanium and Its Alloys For Dental ImplantsDokument13 SeitenTitanium and Its Alloys For Dental ImplantsNathan AbbeyNoch keine Bewertungen
- Micro Implant Anchorage in Orthodontics / Orthodontic Courses by Indian Dental AcademyDokument39 SeitenMicro Implant Anchorage in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Dental Implant MaterialDokument16 SeitenDental Implant MaterialrachmadyNoch keine Bewertungen
- Debate Over Delayed vs. Immediate ImplantsDokument1 SeiteDebate Over Delayed vs. Immediate ImplantsDentalLearningNoch keine Bewertungen
- Extraction of Medical Plastics: Standard Practice ForDokument4 SeitenExtraction of Medical Plastics: Standard Practice FormmorozoNoch keine Bewertungen
- Din en Iso 10360-9 - 2014-04Dokument26 SeitenDin en Iso 10360-9 - 2014-04gviola1405Noch keine Bewertungen
- Titanium Dental Implant SurfacesDokument5 SeitenTitanium Dental Implant SurfacesHugo NeriNoch keine Bewertungen
- SBSI CoagulationDokument3 SeitenSBSI Coagulationjay primaNoch keine Bewertungen
- Is 13726 2002Dokument19 SeitenIs 13726 2002john23141Noch keine Bewertungen
- Comparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Dokument7 SeitenComparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Alex BurdeNoch keine Bewertungen
- Zoje ZJ-W562Dokument63 SeitenZoje ZJ-W562jhonatan garciaNoch keine Bewertungen
- ISO MethodDokument3 SeitenISO MethodMuhammad GhufronNoch keine Bewertungen
- Management of Dry SocketDokument4 SeitenManagement of Dry SocketFakhrul ImamNoch keine Bewertungen
- Zimmer STP, Swot Analysis English: Zimmer Holdings Parent Company Zimmer Holdings Category Sector Tagline/ SloganDokument3 SeitenZimmer STP, Swot Analysis English: Zimmer Holdings Parent Company Zimmer Holdings Category Sector Tagline/ SloganEva Puspita VaniNoch keine Bewertungen
- Oven ManualDokument28 SeitenOven ManualromwellNoch keine Bewertungen
- Titanium Literature ReviewDokument39 SeitenTitanium Literature Reviewapi-570207350Noch keine Bewertungen
- Manual Cementado IndirectoDokument42 SeitenManual Cementado IndirectoLiliana Aguilar VillarrealNoch keine Bewertungen
- Study Materials On Needles PDFDokument24 SeitenStudy Materials On Needles PDFzilangamba_s4535Noch keine Bewertungen
- Distraction KLSDokument54 SeitenDistraction KLSKarim Mohamed100% (1)
- 55 Selection of Appropriate Internal Process Challenge Devices PCDsDokument4 Seiten55 Selection of Appropriate Internal Process Challenge Devices PCDsRakeshNoch keine Bewertungen
- Biological Evaluation of Medical Devices / Biosafety: Applicable ProductsDokument5 SeitenBiological Evaluation of Medical Devices / Biosafety: Applicable ProductsAnonymous iqoU1mtNoch keine Bewertungen
- PFC RP Surgical Technique (DePuy)Dokument43 SeitenPFC RP Surgical Technique (DePuy)Sagaram Shashidar100% (1)
- Software Verification and ValidationDokument27 SeitenSoftware Verification and ValidationkingraajaNoch keine Bewertungen
- In Uence of The Implant Drill Design and SequenceDokument29 SeitenIn Uence of The Implant Drill Design and SequenceHarsha ReddyNoch keine Bewertungen
- P 40 k2 2 en - QD55x QE55x Motor Drive Instruction Manual - Pfaff Electronic Stop - FreeDokument32 SeitenP 40 k2 2 en - QD55x QE55x Motor Drive Instruction Manual - Pfaff Electronic Stop - FreealeXak Noe100% (1)
- Surgical Manual - PremiumDokument80 SeitenSurgical Manual - PremiumJadranka DjorgievaNoch keine Bewertungen
- 99MAD014M4 Digimatic CaliperDokument2 Seiten99MAD014M4 Digimatic CaliperermankurNoch keine Bewertungen
- PFC Sigma KneeDokument36 SeitenPFC Sigma KneeKaustubh KeskarNoch keine Bewertungen
- ASTM F 382 Experiment - 1 - FoyDokument2 SeitenASTM F 382 Experiment - 1 - FoyLucas MlbNoch keine Bewertungen
- As 1386.5-1989 Clean Rooms and Clean Workstations Clean WorkstationsDokument5 SeitenAs 1386.5-1989 Clean Rooms and Clean Workstations Clean WorkstationsSAI Global - APACNoch keine Bewertungen
- Dental Implants PerioDokument54 SeitenDental Implants PerioFourthMolar.com0% (1)
- Medical Coating Innovations - NEW PDFDokument2 SeitenMedical Coating Innovations - NEW PDFleonardq1Noch keine Bewertungen
- Test FixtureDokument6 SeitenTest FixtureSiti Maryam KazimNoch keine Bewertungen
- Straumann® Guided Surgery System InstrumentsDokument48 SeitenStraumann® Guided Surgery System InstrumentsSupaluk Mod ChuencheepNoch keine Bewertungen
- Dental Implant Training EbookDokument21 SeitenDental Implant Training EbookTeodora BadiuNoch keine Bewertungen
- Amvex Intermittent Vacuum Regulator Manual PDFDokument4 SeitenAmvex Intermittent Vacuum Regulator Manual PDFPeter ayalaNoch keine Bewertungen
- Wipak Steriking Sterilization Pouches and RollsDokument4 SeitenWipak Steriking Sterilization Pouches and RollsAnonymous tbJ24554Noch keine Bewertungen
- ANKYLOS Laboratory ManualDokument100 SeitenANKYLOS Laboratory ManualheycoolalexNoch keine Bewertungen
- American Academy of Orthotists & ProsthetistsDokument14 SeitenAmerican Academy of Orthotists & ProsthetistsAndres UlloaNoch keine Bewertungen
- Precision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerDokument8 SeitenPrecision of Intraoral Digital Dental Impressions With ITero and Extraoral Digitization With The ITero and A Model ScannerAlex BurdeNoch keine Bewertungen
- Tracheostomy Suction V LiverpoolDokument3 SeitenTracheostomy Suction V LiverpoolKelvin LoNoch keine Bewertungen
- Stryker Variax Fibula OTDokument24 SeitenStryker Variax Fibula OTDan IonescuNoch keine Bewertungen
- ISO - 80369 - Luers TestingDokument4 SeitenISO - 80369 - Luers TestingFrancescNoch keine Bewertungen
- MHD 01 Surgical Instruments Programme of WorkDokument95 SeitenMHD 01 Surgical Instruments Programme of WorkGana PathiNoch keine Bewertungen
- Enteral Feeding Devices With A Retention Balloon: Standard Test Methods ForDokument7 SeitenEnteral Feeding Devices With A Retention Balloon: Standard Test Methods ForAhmad Zubair RasulyNoch keine Bewertungen
- GD&T BasicsDokument27 SeitenGD&T BasicsfreelanNoch keine Bewertungen
- Sae Geia-Std-0010a-2018Dokument104 SeitenSae Geia-Std-0010a-2018wodonit136100% (1)
- Toshiba Biopsy Guide Adapters PD - MPDUS0006EAIDokument20 SeitenToshiba Biopsy Guide Adapters PD - MPDUS0006EAIJorge FiserNoch keine Bewertungen
- As 4369.2-1996 Surgical Dressings General Purpose Single-Use Woven Gauze SwabsDokument6 SeitenAs 4369.2-1996 Surgical Dressings General Purpose Single-Use Woven Gauze SwabsSAI Global - APACNoch keine Bewertungen
- Industrial Sewing Machine Clutch Motor SpecsDokument15 SeitenIndustrial Sewing Machine Clutch Motor SpecsArja'un TeaNoch keine Bewertungen
- Film Test ValidationDokument19 SeitenFilm Test Validationjerobu100% (1)
- List of Medical Device StandardsDokument5 SeitenList of Medical Device StandardsIsmail YusofNoch keine Bewertungen
- Mecmesin Solutions For Medical DevicesDokument8 SeitenMecmesin Solutions For Medical DevicesPremNoch keine Bewertungen
- As 2145-2002 Stainless Steel Needle Tubing For Manufacture of Medical DevicesDokument8 SeitenAs 2145-2002 Stainless Steel Needle Tubing For Manufacture of Medical DevicesSAI Global - APACNoch keine Bewertungen
- 2008 DilekDokument8 Seiten2008 DilekKaro Polo KnoNoch keine Bewertungen
- Isolation and Char of Amnion and Chorion MSCsDokument10 SeitenIsolation and Char of Amnion and Chorion MSCsÁgnes KocsisNoch keine Bewertungen
- Human Mesenchymal Stem Cells - Current Trends and Future ProspectiveDokument18 SeitenHuman Mesenchymal Stem Cells - Current Trends and Future ProspectiveÁgnes KocsisNoch keine Bewertungen
- Human Mesenchymal Stem Cells - Current Trends and Future ProspectiveDokument17 SeitenHuman Mesenchymal Stem Cells - Current Trends and Future ProspectiveÁgnes KocsisNoch keine Bewertungen
- Human Mesenchymal Stem Cells - Current Trends and Future ProspectiveDokument18 SeitenHuman Mesenchymal Stem Cells - Current Trends and Future ProspectiveÁgnes KocsisNoch keine Bewertungen
- Microtubules and Centrosomes PDFDokument11 SeitenMicrotubules and Centrosomes PDFÁgnes KocsisNoch keine Bewertungen
- Crisfield M A Vol 2 Non-Linear Finite Element Analysis of Solids and Structures Advanced TopicsDokument509 SeitenCrisfield M A Vol 2 Non-Linear Finite Element Analysis of Solids and Structures Advanced TopicsIffat Siddqiue0% (1)
- G.D.GOENKA PUBLIC SCHOOL CLASS 10 CHEMISTRY CHAPTER 2 ACIDS BASES SALTS ASSIGNMENTDokument3 SeitenG.D.GOENKA PUBLIC SCHOOL CLASS 10 CHEMISTRY CHAPTER 2 ACIDS BASES SALTS ASSIGNMENTvikas aggarwal100% (1)
- E401Dokument4 SeitenE401Katrina BucudNoch keine Bewertungen
- Grade 9: Coordinate GeometryDokument5 SeitenGrade 9: Coordinate GeometryEduGainNoch keine Bewertungen
- ASTM TablesDokument185 SeitenASTM Tableslahiru198367% (3)
- Meclizine HCLDokument10 SeitenMeclizine HCLChEng_Noch keine Bewertungen
- Chapter 1 Lecture1Dokument39 SeitenChapter 1 Lecture1Anonymous AFFiZnNoch keine Bewertungen
- Physics Module Form 4 Chapter 3 Forces & PressureDokument25 SeitenPhysics Module Form 4 Chapter 3 Forces & PressureMisratul A'la Mahyuddin100% (2)
- Composite MaterialsDokument278 SeitenComposite Materialsjaddddd100% (8)
- Gear Motors: Achieving The Perfect Motor & Gearbox MatchDokument16 SeitenGear Motors: Achieving The Perfect Motor & Gearbox MatchJohn LeeNoch keine Bewertungen
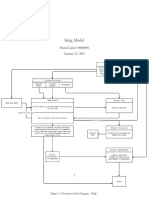
- Ising ModelDokument5 SeitenIsing Modeldecerto252Noch keine Bewertungen
- Reka Bentuk, Pembinaan Dan Pentadbiran UjianDokument9 SeitenReka Bentuk, Pembinaan Dan Pentadbiran UjianAiman HazimNoch keine Bewertungen
- Especificacion SHY73MC4 UDokument3 SeitenEspecificacion SHY73MC4 UYgor Salgado100% (3)
- Adaptive Followup Mastering PhysicsDokument8 SeitenAdaptive Followup Mastering PhysicsElloani Ross Arcenal PitogoNoch keine Bewertungen
- Astm D 1746 97 TH 2002 PDFDokument5 SeitenAstm D 1746 97 TH 2002 PDFJed BrionesNoch keine Bewertungen
- Determining Height with a TransitDokument6 SeitenDetermining Height with a TransitMNoch keine Bewertungen
- Biological Effect and Medical Applications of Electromagnetic EnergyDokument580 SeitenBiological Effect and Medical Applications of Electromagnetic EnergyTienRienNoch keine Bewertungen
- Composites of Polymer and Orange PeelDokument7 SeitenComposites of Polymer and Orange PeelkarthiNoch keine Bewertungen
- (Architecture Ebook) Alvar Aalto, Alvar Aalto and The Bio-ArchitectureDokument5 Seiten(Architecture Ebook) Alvar Aalto, Alvar Aalto and The Bio-Architecturepooh86poohNoch keine Bewertungen
- Conduction, Convection, & RadiationDokument14 SeitenConduction, Convection, & Radiationyuvionfire100% (1)
- Plate Bending Element Formulation and Stiffness Matrix DevelopmentDokument6 SeitenPlate Bending Element Formulation and Stiffness Matrix DevelopmentSeyhan ÖzenNoch keine Bewertungen
- OSHA Confined Space Standards and HazardsDokument93 SeitenOSHA Confined Space Standards and HazardsPrimelift Safety Resources LimitedNoch keine Bewertungen
- History of Contingency Theory: Reporter: Emiliana J. LozanoDokument23 SeitenHistory of Contingency Theory: Reporter: Emiliana J. Lozanoaireenclores100% (3)
- Steam Drum Design CalsDokument78 SeitenSteam Drum Design Calsabdulrehmandescon100% (1)
- Sedimentary Geology 188-189 (2006) 357 - 378Dokument22 SeitenSedimentary Geology 188-189 (2006) 357 - 378dvrmtNoch keine Bewertungen
- Cement Chapter 4Dokument11 SeitenCement Chapter 4shani5573100% (2)
- Static Studies of Magneto-Electro-Elastic 3-D Beam Using ANSYS - FINALDokument8 SeitenStatic Studies of Magneto-Electro-Elastic 3-D Beam Using ANSYS - FINALjssrikantamurthyNoch keine Bewertungen
- Turbocharger Test GuidelinesDokument13 SeitenTurbocharger Test Guidelinespardomu0% (1)
- Forensic Chemistry ToxicologyDokument139 SeitenForensic Chemistry ToxicologyCeasar Estrada94% (18)
- Free Electron Theory 2015-16 (VTU) PDFDokument14 SeitenFree Electron Theory 2015-16 (VTU) PDFU and me SNoch keine Bewertungen
- Learning from Lectures: Learning from lectures, listening & notetaking skillsVon EverandLearning from Lectures: Learning from lectures, listening & notetaking skillsBewertung: 5 von 5 Sternen5/5 (6)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningVon EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningBewertung: 4.5 von 5 Sternen4.5/5 (55)
- The Everything Guide to Study Skills: Strategies, tips, and tools you need to succeed in school!Von EverandThe Everything Guide to Study Skills: Strategies, tips, and tools you need to succeed in school!Bewertung: 4.5 von 5 Sternen4.5/5 (6)
- 700 Driving Theory Test Questions & Answers: Updated Study Guide With Over 700 Official Style Practise Questions For Cars - Based Off the Highway CodeVon Everand700 Driving Theory Test Questions & Answers: Updated Study Guide With Over 700 Official Style Practise Questions For Cars - Based Off the Highway CodeNoch keine Bewertungen
- Math Olympiad Contests Preparation For Grades 4-8: Competition Level Math for Middle School Students to Win MathCON, AMC-8, MATHCOUNTS, and Math LeaguesVon EverandMath Olympiad Contests Preparation For Grades 4-8: Competition Level Math for Middle School Students to Win MathCON, AMC-8, MATHCOUNTS, and Math LeaguesNoch keine Bewertungen
- A-level Maths Revision: Cheeky Revision ShortcutsVon EverandA-level Maths Revision: Cheeky Revision ShortcutsBewertung: 3.5 von 5 Sternen3.5/5 (8)
- TEF Canada Expression Écrite : 150 Topics To SucceedVon EverandTEF Canada Expression Écrite : 150 Topics To SucceedBewertung: 4.5 von 5 Sternen4.5/5 (17)
- ATI TEAS Study Guide: The Most Comprehensive and Up-to-Date Manual to Ace the Nursing Exam on Your First Try with Key Practice Questions, In-Depth Reviews, and Effective Test-Taking StrategiesVon EverandATI TEAS Study Guide: The Most Comprehensive and Up-to-Date Manual to Ace the Nursing Exam on Your First Try with Key Practice Questions, In-Depth Reviews, and Effective Test-Taking StrategiesNoch keine Bewertungen
- PSI National Real Estate License Exam Prep 2020-2021: A Study Guide with 550 Test Questions and Answers Explanations (Includes Practice Tests for Brokers and Salespersons)Von EverandPSI National Real Estate License Exam Prep 2020-2021: A Study Guide with 550 Test Questions and Answers Explanations (Includes Practice Tests for Brokers and Salespersons)Bewertung: 1 von 5 Sternen1/5 (1)
- IELTS Speaking Vocabulary Builder (Band 5-6): Master Phrases and Expressions for the IELTS Speaking ExamVon EverandIELTS Speaking Vocabulary Builder (Band 5-6): Master Phrases and Expressions for the IELTS Speaking ExamBewertung: 5 von 5 Sternen5/5 (1)
- 71 Ways to Practice English Reading: Tips for ESL/EFL LearnersVon Everand71 Ways to Practice English Reading: Tips for ESL/EFL LearnersBewertung: 5 von 5 Sternen5/5 (2)
- 1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideVon Everand1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideBewertung: 3.5 von 5 Sternen3.5/5 (7)
- BCBA Exam Prep A Study Guide to Practice Test Questions With Answers and Master the Board Certified Behavior Analyst ExaminationVon EverandBCBA Exam Prep A Study Guide to Practice Test Questions With Answers and Master the Board Certified Behavior Analyst ExaminationNoch keine Bewertungen
- Real Stories: The All-Inclusive Textbook for Developmental Writing and ReadingVon EverandReal Stories: The All-Inclusive Textbook for Developmental Writing and ReadingNoch keine Bewertungen
- The LearnCurious Companion to the Digital SAT: VerbalVon EverandThe LearnCurious Companion to the Digital SAT: VerbalNoch keine Bewertungen
- Master the Public Safety Dispatcher/911 Operator ExamVon EverandMaster the Public Safety Dispatcher/911 Operator ExamBewertung: 5 von 5 Sternen5/5 (1)