Das könnte Ihnen auch gefallen
- 1 s2.0 S2451993617300270 Main PDFDokument6 Seiten1 s2.0 S2451993617300270 Main PDFIndahEkaPutriNoch keine Bewertungen
- Iridocorneal Endothelial Syndrome in A 16-Year-OldDokument4 SeitenIridocorneal Endothelial Syndrome in A 16-Year-OldCamiCasasNoch keine Bewertungen
- Is Episcleritis Associated To Glaucoma?Dokument3 SeitenIs Episcleritis Associated To Glaucoma?Alvin JulianNoch keine Bewertungen
- Cystoid Macular EdemaDokument5 SeitenCystoid Macular EdemaAgnes Triana BasjaNoch keine Bewertungen
- Secondary Buphthalmos: A Case SeriesDokument2 SeitenSecondary Buphthalmos: A Case SeriesdrheriNoch keine Bewertungen
- Indications Vitrectomy Retinoschisis: For CongenitalDokument5 SeitenIndications Vitrectomy Retinoschisis: For CongenitalRohamonangan TheresiaNoch keine Bewertungen
- A Case Report On A Rare Posterior Type of Persistent Fetal VasculatureDokument3 SeitenA Case Report On A Rare Posterior Type of Persistent Fetal VasculaturevaleskaliNoch keine Bewertungen
- Granuloma PiogenikDokument2 SeitenGranuloma PiogenikVindhiya Lissa VioletthaNoch keine Bewertungen
- GlaucomaDokument18 SeitenGlaucomaOncología CdsNoch keine Bewertungen
- Mcculley 2012Dokument11 SeitenMcculley 2012Luisa Mayta PitmanNoch keine Bewertungen
- 100255-Article Text-1482-2-10-20220311Dokument6 Seiten100255-Article Text-1482-2-10-20220311Fachry RahmanNoch keine Bewertungen
- Diagnosis BandingDokument10 SeitenDiagnosis BandingIntan Rahmi NasyaNoch keine Bewertungen
- Spontaneous Resolution of Ophthalmologic Symptoms Following Bilateral Traumatic Carotid Cavernous FistulaeDokument6 SeitenSpontaneous Resolution of Ophthalmologic Symptoms Following Bilateral Traumatic Carotid Cavernous FistulaeMaria Angelina BunawanNoch keine Bewertungen
- Exudative Retinopathy of Adults A Late S PDFDokument5 SeitenExudative Retinopathy of Adults A Late S PDFInna BujorNoch keine Bewertungen
- Phthisis Bulbi: Clinical and Pathologic Findings in RetinoblastomaDokument6 SeitenPhthisis Bulbi: Clinical and Pathologic Findings in RetinoblastomaEstmar ValentinoNoch keine Bewertungen
- Complications in UveitisVon EverandComplications in UveitisFrancesco PichiNoch keine Bewertungen
- Primary Open-Angle Glaucoma: SeminarDokument10 SeitenPrimary Open-Angle Glaucoma: SeminarFebry LuthunananaNoch keine Bewertungen
- RiddlesDokument44 SeitenRiddlessafasayed100% (1)
- A Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeDokument3 SeitenA Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeSriana K. LaliyoNoch keine Bewertungen
- Orbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusDokument4 SeitenOrbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusYosiita KartinaaNoch keine Bewertungen
- Clinical CasesDokument49 SeitenClinical Casesnorfitri hadeyNoch keine Bewertungen
- Bilateral Secondary Glaucoma and Systemic Hypertension in Marfan'S SyndromeDokument5 SeitenBilateral Secondary Glaucoma and Systemic Hypertension in Marfan'S SyndromeFriskadoreendaputriNoch keine Bewertungen
- 2005 Entropion CongenitalDokument2 Seiten2005 Entropion Congenitalsaraya amajidaNoch keine Bewertungen
- Advanced Glaukoma As A Late Manifestation in Axenfeld-Rieger SyndromeDokument8 SeitenAdvanced Glaukoma As A Late Manifestation in Axenfeld-Rieger SyndromeollyNoch keine Bewertungen
- Optic Neuritis in Leprosy - 231215 - 030338Dokument2 SeitenOptic Neuritis in Leprosy - 231215 - 030338dr samyNoch keine Bewertungen
- American Journal of Ophthalmology Case ReportsDokument3 SeitenAmerican Journal of Ophthalmology Case ReportsElison Jaya PanggaloNoch keine Bewertungen
- Retninal Vein OcclusionDokument10 SeitenRetninal Vein OcclusionuhibNoch keine Bewertungen
- Acknowledgement: Aniridia Associated With Congenital Aphakia and Secondary GlaucomaDokument3 SeitenAcknowledgement: Aniridia Associated With Congenital Aphakia and Secondary GlaucomaNisrina FarihaNoch keine Bewertungen
- Congenital Ptosis - JurnalDokument28 SeitenCongenital Ptosis - JurnalJohanes Arie SetiawanNoch keine Bewertungen
- Case Reports: Acute Haptic-Induced Ciliary Sulcus Irritation Associated With Single-Piece Acrysof Intraocular LensesDokument7 SeitenCase Reports: Acute Haptic-Induced Ciliary Sulcus Irritation Associated With Single-Piece Acrysof Intraocular Lensescome puritosNoch keine Bewertungen
- Ostiogenesis ImperfectaDokument4 SeitenOstiogenesis Imperfectamarlon GarcíaNoch keine Bewertungen
- Essential Infantile Esotropia An Unusual Case ReportDokument3 SeitenEssential Infantile Esotropia An Unusual Case ReportInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Spontaneous Anterior Lens Capsular Dehiscence Causing Lens Particle GlaucomaDokument3 SeitenSpontaneous Anterior Lens Capsular Dehiscence Causing Lens Particle GlaucomaKakak AdekNoch keine Bewertungen
- Management of Double-Penetrating Ocular Injury With Retained Intraorbital Metallic Foreign BodyDokument4 SeitenManagement of Double-Penetrating Ocular Injury With Retained Intraorbital Metallic Foreign BodyShirakawa AlmiraNoch keine Bewertungen
- Journal Casereport 1Dokument5 SeitenJournal Casereport 1Arif MohammadNoch keine Bewertungen
- Herpes Zoster OphthalmicusDokument12 SeitenHerpes Zoster OphthalmicusGio Vano NaihonamNoch keine Bewertungen
- Esferofauia Aislada y GlaucomaDokument3 SeitenEsferofauia Aislada y GlaucomaManuel VasquezNoch keine Bewertungen
- Intraocular Lens Subluxation in Marfan SyndromeDokument3 SeitenIntraocular Lens Subluxation in Marfan SyndromeSusPa NarahaNoch keine Bewertungen
- MainDokument7 SeitenMainSyeda F AmbreenNoch keine Bewertungen
- Laporan Kasus NeurooftalmologiDokument12 SeitenLaporan Kasus NeurooftalmologiPradistya Syifa YudiasariNoch keine Bewertungen
- Cambridge Ophthalmological SymposiumDokument22 SeitenCambridge Ophthalmological SymposiumvericaNoch keine Bewertungen
- Dafpus 10 Sympathetic - Opthalmia-2Dokument7 SeitenDafpus 10 Sympathetic - Opthalmia-2Anonymous jh87ryNoch keine Bewertungen
- Congenital PtosisDokument15 SeitenCongenital PtosisRobiniskandarNoch keine Bewertungen
- Vaskulitis ChorioretinopathyDokument10 SeitenVaskulitis ChorioretinopathydrheriNoch keine Bewertungen
- Retinal Tear: An Unusual Complication of Ocular ToxoplasmosisDokument5 SeitenRetinal Tear: An Unusual Complication of Ocular ToxoplasmosisMuhammad Irfan FaizNoch keine Bewertungen
- Case Review - EndophthalmitisDokument4 SeitenCase Review - EndophthalmitisDr Shawgat Ul Karim KhanNoch keine Bewertungen
- Retinoblastoma PDFDokument5 SeitenRetinoblastoma PDFRiska PermatasariNoch keine Bewertungen
- Skew Deviation RevisitedDokument24 SeitenSkew Deviation RevisitedPriscila Verduzco MartínezNoch keine Bewertungen
- Uveitis 2Dokument9 SeitenUveitis 2srihandayaniakbarNoch keine Bewertungen
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDokument5 SeitenHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Mechanisms of Visual Loss in PapilledemaDokument8 Seiten(10920684 - Neurosurgical Focus) Mechanisms of Visual Loss in PapilledemaYusuf BrilliantNoch keine Bewertungen
- AAO Network UveitisDokument72 SeitenAAO Network UveitisSafa Abdualrahaman Ali HamadNoch keine Bewertungen
- Simple Ectopia Lentis A Case ReportDokument17 SeitenSimple Ectopia Lentis A Case ReportSyeda F AmbreenNoch keine Bewertungen
- Glaucoma, Pseudoexfoliation: Emedicine Specialtiesophthalmologyintraocular PressureDokument9 SeitenGlaucoma, Pseudoexfoliation: Emedicine Specialtiesophthalmologyintraocular PressureChintya Dwi PutriNoch keine Bewertungen
- Congenital Ptosis Case PresentationDokument8 SeitenCongenital Ptosis Case PresentationHitesh Sharma67% (3)
- Diagnosis and Management of Malignant GlaucomaDokument3 SeitenDiagnosis and Management of Malignant GlaucomaYazmin Peñaloza RoaNoch keine Bewertungen
- Eye RoundsDokument5 SeitenEye RoundsVitazty GustavitaNoch keine Bewertungen
- Congenital Ptosis - GenetikaDokument28 SeitenCongenital Ptosis - GenetikaJohanes Arie SetiawanNoch keine Bewertungen
- Eye Net Magazine Aao: Pathogenesis/MechanismDokument4 SeitenEye Net Magazine Aao: Pathogenesis/MechanismDelila MaharaniNoch keine Bewertungen
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Von EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Noch keine Bewertungen
- Coccygectomy For Stubborn CoccydyniaDokument4 SeitenCoccygectomy For Stubborn CoccydyniaDiaz RandanilNoch keine Bewertungen
- Surgical Technique of CoccygectomyDokument7 SeitenSurgical Technique of CoccygectomyDiaz RandanilNoch keine Bewertungen
- Congenital: Ectropion AND DistichiasisDokument38 SeitenCongenital: Ectropion AND DistichiasisDiaz RandanilNoch keine Bewertungen
- Lateral RhinotomyDokument11 SeitenLateral RhinotomyDiaz RandanilNoch keine Bewertungen
- Medial Ectropion Repair of Lower Eyelids With A Cicatricial ComponentDokument3 SeitenMedial Ectropion Repair of Lower Eyelids With A Cicatricial ComponentDiaz RandanilNoch keine Bewertungen
- 11.ok-Lap. Kas. Dr. IqbalaDokument2 Seiten11.ok-Lap. Kas. Dr. IqbalaDiaz RandanilNoch keine Bewertungen
- Background: FrequencyDokument2 SeitenBackground: FrequencyDiaz RandanilNoch keine Bewertungen
- Surgery Department Medical Faculty Yarsi University Jakarta 2008Dokument17 SeitenSurgery Department Medical Faculty Yarsi University Jakarta 2008Diaz RandanilNoch keine Bewertungen
- Entropion and Ectropion Repair: BackgroundDokument10 SeitenEntropion and Ectropion Repair: BackgroundDiaz RandanilNoch keine Bewertungen
- Elements - Digital Painting Tutorial Series Vol1Dokument70 SeitenElements - Digital Painting Tutorial Series Vol1castagineNoch keine Bewertungen
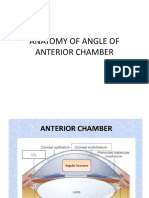
- Anatomy of Angle of Anterior ChamberDokument67 SeitenAnatomy of Angle of Anterior ChamberRahnaNoch keine Bewertungen
- Iris Recognition After DeathDokument14 SeitenIris Recognition After DeathragouNoch keine Bewertungen
- Ch. 15 Sensory SystemDokument23 SeitenCh. 15 Sensory SystemJackieFernandezNoch keine Bewertungen
- Biology Textbook Part 1 English Medium - Kerala STD 10Dokument72 SeitenBiology Textbook Part 1 English Medium - Kerala STD 10Sreelakshmi PMNoch keine Bewertungen
- 01 Amali Sci F2Dokument34 Seiten01 Amali Sci F2Nur Dalila YusofNoch keine Bewertungen
- Slit Lamp Examination: by DR - Pragnya RaoDokument43 SeitenSlit Lamp Examination: by DR - Pragnya RaoPragnya Rao Donthineni80% (5)
- Uveal TractDokument56 SeitenUveal Tractmaf manNoch keine Bewertungen
- G3 - Q2 LC 1 2 1Dokument5 SeitenG3 - Q2 LC 1 2 1Churchel E. GlodoveNoch keine Bewertungen
- TumorDokument8 SeitenTumorputyCeria86Noch keine Bewertungen
- Special Senses: Part I: The Eye and VisionDokument8 SeitenSpecial Senses: Part I: The Eye and VisionJoanna Carla Marmonejo Estorninos-WalkerNoch keine Bewertungen
- Glaucoma GuidelinesDokument28 SeitenGlaucoma GuidelinesRina RostianaNoch keine Bewertungen
- Ocular InjuriesDokument66 SeitenOcular InjuriesSanatan JaniNoch keine Bewertungen
- ColorsDokument5 SeitenColorsSafeer IqbalNoch keine Bewertungen
- CONCORDokument13 SeitenCONCORSaumya Sankar RayNoch keine Bewertungen
- Oncology of The Eye and AdnexaDokument167 SeitenOncology of The Eye and Adnexadidier dedziNoch keine Bewertungen
- The Basics of Iridology 3 - Markings by Francesco PuerariDokument303 SeitenThe Basics of Iridology 3 - Markings by Francesco PuerariAmit KapoorNoch keine Bewertungen
- Continuum Neuro-OphthalmologyDokument361 SeitenContinuum Neuro-Ophthalmologyluizmiranda108Noch keine Bewertungen
- Drawing and Painting Anime and Manga Faces - Step-By-Step Techniques For Creating Authentic Characters and Expressions (2021, Nao Yazawa)Dokument370 SeitenDrawing and Painting Anime and Manga Faces - Step-By-Step Techniques For Creating Authentic Characters and Expressions (2021, Nao Yazawa)Whitney Cartwright100% (3)
- Ophthalmology PDFDokument92 SeitenOphthalmology PDFMarwa AhmedNoch keine Bewertungen
- AAB Eye Anatomy Coloring WorksheetDokument2 SeitenAAB Eye Anatomy Coloring Worksheetsachd16100% (2)
- IRIS Recognition Technique Through Douglas MethodDokument27 SeitenIRIS Recognition Technique Through Douglas MethodVidya MoolyaNoch keine Bewertungen
- HifemaDokument7 SeitenHifemawidirayNoch keine Bewertungen
- OCTA InflammatoryEyediseaseSrivastavaDokument24 SeitenOCTA InflammatoryEyediseaseSrivastavaPriyanka DocNoch keine Bewertungen
- Senses HandoutsDokument13 SeitenSenses HandoutsxylentknightNoch keine Bewertungen
- Chapter 1: Introduction: 1.1 BiometricsDokument10 SeitenChapter 1: Introduction: 1.1 BiometricsAnkur KumarNoch keine Bewertungen
- Iridology: (Introduction)Dokument27 SeitenIridology: (Introduction)OgooNkemNoch keine Bewertungen
- IridENews5 PDFDokument20 SeitenIridENews5 PDFmalin.oloierNoch keine Bewertungen
- 14 Nervous SystemDokument89 Seiten14 Nervous SystemJose LunaNoch keine Bewertungen
- Physical Assessment Guide To Collect Objective Client DataDokument13 SeitenPhysical Assessment Guide To Collect Objective Client DatagabbyNoch keine Bewertungen